Family Planning Programme in Nepal

Introduction
Family planning has been a key priority programme of the Government of Nepal. Recognized by the United Nations in 1967, the government incorporated family planning into its national plan as early as 1966. However, the movement for family planning in Nepal started even earlier, in 1959, under the Nepal Medical Association. That same year, it became an associate member of the International Planned Parenthood Federation (IPPF).
Initially, the primary activities of the association focused on communication strategies to raise awareness among people about the importance and concept of family planning. The implementation of the family planning programme was deemed essential not only to safeguard the health and welfare of mothers, children, and entire families but also to establish a balance between population growth and the country’s economic development.
Among the 1.9 billion women of reproductive age (15–49 years) worldwide in 2021, 1.1 billion had a need for family planning. Of these, 874 million were using modern contraceptive methods, while 164 million faced an unmet need for contraception. The proportion of family planning needs satisfied by modern methods, measured as Sustainable Development Goals (SDG) Indicator 3.7.1, has stagnated globally at around 77% from 2015 to 2022. However, progress has been observed in sub-Saharan Africa, where the satisfaction rate increased from 52% to 58% during the same period. Notably, condoms are the only contraceptive method that prevents both pregnancy and the transmission of sexually transmitted infections (STIs), including HIV. The use of contraception also promotes human rights, empowering individuals to determine the number and spacing of their children. In 2022, the global contraceptive prevalence rate was estimated at 65% for any method and 58.7% for modern methods among married or in-union women.
According to the Census Report 2021, Nepal’s population has reached 29,192,480, reflecting an increase of 2,697,976 compared to 26,494,504 in 2011, marking a decade-long growth rate of 10.18%. Despite this growth, Nepal’s fertility rate has seen a significant decline, dropping from 2.516 in 2011 to 1.853 in 2021. This rapid decline highlights the success of sustained efforts by the Government of Nepal and partner organizations to stabilize the population. However, population growth is expected to continue until the fertility rate reaches the replacement level. Among currently married women, 57% are using some form of contraception, with 43% relying on modern methods and 15% on traditional methods. The most commonly used modern methods include female sterilization (13%), injectables (9%), and implants (6%). Among traditional methods, withdrawal is the most prevalent, used by 13% of married women, followed by the rhythm method, used by 2%.
Over the years, the use of any family planning method among currently married women has increased significantly, rising from 29% in 1996 to 57% in 2022. However, the use of modern contraceptive methods, which increased from 26% in 1996 to 44% in 2006, has remained stagnant at 43% from 2011 through 2022. This stagnation indicates the need for renewed efforts to achieve Nepal’s Sustainable Development Goal (SDG) target under indicator 3.7.1(a), which aims for 53% of women of reproductive age to use modern contraceptive methods by 2022 and 60% by 2030. These trends emphasize the importance of enhancing access to family planning services and raising awareness to address unmet needs and meet national targets.
Definition of Family Planning
(According to WHO Expert Committee, 1971) “Family planning is a way of thinking & living that is adapted voluntary upon the basis of knowledge, attitude & responsible decisions by individuals and couples in order to promote the health and welfare of the family group and thus contribute effectively to the social development of a country”.
James Allman. “The conscious action taken by an individual or couples to regulate the number and spacing of their children in accordance with their personal preferences”.
Objectives of Family Planning
- To avoid unwanted birth
- To bring about wanted birth
- To regulate the interval between pregnancy
- To control the time at which birth occur in relation to age of parent
- To determine the number of children in the family
- To provide treatment in case of infertility in couples
- To improve and promote the health status of mothers’ children as well as whole family.
- To decrease the maternal and child mortality and morbidity rate.
Scope of Family Planning
WHO expert committee (1970) has stated that family planning is its preview.
- The proper spacing and limitation of births
- Advice on sterility
- Education for parenthood
- Sex education
- Screening for pathological conditions related to the reproductive system (e.g. cervical cancer)
- Genetic counseling
- Premarital consultation and examination
- Carrying out of pregnancy tests
- Marriage counseling
- The perception of couples for the arrival of their first child
- Providing services for unmarried mothers
- Teaching home economics and nutrition
- Providing adoptive services.
These activities vary from country to country, depending on national objectives and family planning policies.
Health aspects of Family Planning
- Women’s health and women’s empowerment
- Avoidance of unwanted pregnancies: The primary goal of family planning is to prevent unwanted pregnancies. Unwanted pregnancies may result in induced abortions (including illegal or unsafe abortions), which are among the most dangerous outcomes of such pregnancies. Studies also indicate a higher incidence of mental health disturbances among mothers experiencing unwanted pregnancies.
- Limiting the numbers of births and proper spacing: Repeated pregnancies increase the risk of maternal mortality and morbidity. Conditions such as uterine rupture, uterine atony, toxemia, placenta previa, and anemia are common among mothers with high parity. Additionally, the rate of stillbirths tends to rise significantly with an increased number of pregnancies. Family planning (FP) is the most effective method to limit family size and regulate the intervals between births, thereby improving maternal health.
- Timing the births particularly the first and last in relation to the age of the mother: Mothers generally face a higher risk of mortality below the age of 20 and above the age of 30 to 35.
2. Fetal Health
Family planning allows couples to avoid unwanted pregnancies, reducing the risk of genetic abnormalities, such as Down syndrome, which are more common with advancing maternal age. Low birth weight (LBW) infants, often resulting from premature births or inadequate fetal nutrition, are less likely to thrive, more prone to illness, and four times more likely to die within the first year of life compared to babies with normal weight. Therefore, family planning encourages spacing pregnancies at least two years apart to promote healthier fetal outcomes.
3. Infant and Child Health
Family planning (FP) is highly relevant to pediatrics, as it significantly impacts infant and child health. Practicing appropriate family size and birth spacing can yield substantial benefits for child health.
Child mortality: A birth interval of 2 to 3 years is associated with a significant reduction in child mortality rates. This highlights the importance of FP in enhancing the survival of all children within a family.
Child growth, development, and nutrition: Birth spacing and family size are crucial factors in promoting optimal child growth and development. A child in a small family with adequately spaced births is more likely to receive adequate love, care, and nutrition. In this sense, family planning serves as an effective measure to prevent malnutrition.
Infectious diseases: Children in large families are at a higher risk of contracting infectious diseases such as gastroenteritis, respiratory infections, and skin infections due to crowded living conditions.
Intelligence: Studies have shown that children from larger families tend to have lower IQ (intelligence quotient) scores compared to those from smaller families, likely due to resource limitations and reduced individual attention.
Need for Family Planning
Advantages of a small family
- Family Planning starts with marriage at an appropriate age: Marriage should occur at a suitable age to ensure physical and emotional readiness. According to legal and biological standards: Girls should not marry before the age of 18 and boys should not marry before the age of 21.
- Optimal age for pregnancy: For the health and well-being of the mother and child: The safest period for pregnancy is when the mother is between 20 and 30 years of age.
- Maintaining a reasonable gap between children: A proper interval between two pregnancies allows: The mother enough time to restore her body’s nutrients and recover fully from the previous pregnancy.
- Women: Family planning helps women prevent unwanted pregnancies. Since the 1960s, Family Planning programs have supported women globally in avoiding unintended pregnancies. These programs have significantly reduced the risks of maternal mortality due to high-risk pregnancies and unsafe abortions. If all women could avoid high-risk pregnancies, maternal deaths could decrease by one-quarter. Additionally, many Family Planning methods offer other health benefits, such as hormonal methods that help prevent certain types of cancer and condoms that help prevent sexually transmitted infections (STIs), including HIV/AIDS.
Advantages for the mother
- A mother can maintain her health by limiting the number of children and spacing pregnancies appropriately.
- Planning reduces the fear and anxiety associated with unintended pregnancies.
- A smaller number of children minimizes physical and emotional strain on the mother.
- The mother will have more time and energy to provide proper attention, love, and care to her children.
- With fewer responsibilities, the mother can participate in education, vocational training, and community projects.
- A small family enables the mother to explore better job opportunities.
- A planned family reduces the chances of fetal death, birth defects, and mortality during infancy and childhood.
2. Child: Family planning helps save children’s lives by enabling women to space births. If all children were born at least two years apart, millions of deaths could be prevented.
Advantages for the child
- The child will have a conducive environment for proper physical and psychological growth and development.
- The child will receive adequate nutrition, education, parental care, and love.
- A well-planned family allows the child to contribute to establishing a strong economic foundation for the family.
3. Men: Family planning benefits both men and women by enabling them to plan their families effectively. Men worldwide report that family planning allows them to provide a better quality of life for their families.
Advantages for the father
- Fathers can ensure better education, comfort, nutrition, clothing, and recreational opportunities for their children.
- A smaller, planned family reduces stress, allowing fathers to be more relaxed and maintain good health.
- Fathers can enjoy improved living conditions, better health, and increased productivity in the workforce.
4. Family: Family planning enhances the overall well-being of families. Couples with fewer children are better equipped to provide adequate food, clothing, housing, and education for their children, ensuring a higher quality of life for the entire family.
5. Nations/community: Family planning contributes to national development. In countries where women are having fewer children compared to previous generations, economic progress occurs at a faster pace.
Advantages for the community
- Small families help conserve natural resources and increase savings.
- Adopting the small family norm ensures adequate schools, hospitals, and other essential services for everyone.
- It promotes more employment opportunities for the community.
- Small, planned families bring long-term happiness, peace, harmony, and prosperity to society.
6. Earth: Family planning contributes to a sustainable future. By limiting the number of children, the world’s population growth can slow down, preventing it from doubling in less than 50 years.
Advantages for the Earth:
- Reduced population growth helps decrease the strain on natural resources such as water and fertile soil.
- Future generations will face fewer challenges in meeting basic needs, ensuring a better quality of life for everyone.
- A smaller global population enables more equitable distribution of resources and opportunities for a good life.
Types of family planning
A. Temporary family planning methods
I. Behavioral/natural methods
- Lactational Amenorrhea Method (LAM)
- Calendar method
- Cervical mucus method
- Basal body temperature (BBT) method
- Withdrawal method
II. Chemical methods
- Spermicides –Foam, tablet (Kamal chhaki),
- Jelly, paste & cream
III. Mechanical methods
- Condom
- Male condom
- Female condom
2. Diaphragm
3. Cervical cap
4. Intra Uterine Contraceptive Device (IUCD)
IV. Hormonal methods or physiological method
- Oral Contraceptive Pills
- Depo-Provera
- Norplant
B. Permanent family planning/voluntary sterilization
I. Male sterilization (Vasectomy)
II. Female voluntary sterilization
A. Temporary family planning methods
I. Behavioral/natural methods
Behavioral or natural methods of family planning include practices such as avoiding unprotected intercourse during fertile days to prevent pregnancy. These methods rely on understanding the natural fertility cycles of the body and include techniques such as tracking ovulation, monitoring basal body temperature, and observing changes in cervical mucus.
1. Lactational Amenorrhea Method (LAM) : LAM is a natural family planning method based on the natural infertility experienced by breastfeeding women, particularly during the early postpartum months. ‘Lactational’ refers to breastfeeding, while ‘amenorrhea’ signifies the absence of menstruation. When practiced correctly, LAM is an effective temporary contraceptive choice for women. This method highlights self-awareness and comes with no side effects, making it an attractive option for individuals seeking natural, hormone-free approaches to family planning.
Mechanism of action
During breastfeeding, nipple stimulation caused by suckling sends signals to the hypothalamus, triggering a series of hormonal responses. These signals reduce the secretion of gonadotropin-releasing hormone (GnRH), which in turn decreases the release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) from the pituitary gland. This hormonal shift disrupts the development of ovarian follicles, preventing ovulation. Additionally, suckling increases the production of prolactin, a hormone that plays a key role in milk production and further inhibits ovulation. Ovulation remains suppressed as long as breastfeeding is frequent, intense, and consistent. However, in most lactating women, ovulation naturally resumes around six months postpartum, as the frequency and intensity of breastfeeding typically decline.
Effectiveness
The LAM is 98% effective as a contraceptive when the following conditions are met:
- The mother is fully or nearly fully breastfeeding.
- The return of menstrual periods has not occurred.
- The mother is less than 6 months postpartum.
Fully breastfeeding is defined by:
- Breastfeeding whenever the baby desires, with at least one session every 4 hours during the day.
- Providing nighttime feedings, with at least one session every 6 hours.
- Not introducing other foods or fluids in place of a breast milk meal, ensuring exclusive breastfeeding.
Advantages
- Provides effective pregnancy prevention for at least 7 months, with the possibility of longer protection if breastfeeding is frequent both day and night.
- Promotes optimal breastfeeding patterns for the mother and baby.
- Can be used immediately after childbirth without delay.
- Requires no additional supplies or devices for pregnancy prevention.
- Does not have hormonal side effects.
Disadvantages
- Its effectiveness beyond 7 months is not guaranteed.
- Frequent breastfeeding may be inconvenient or challenging, especially for working mothers.
- Does not offer protection against sexually transmitted infections (STIs), including HIV/AIDS.
- If the mother is HIV-positive, there is a small risk of transmitting the virus through breast milk to the baby.
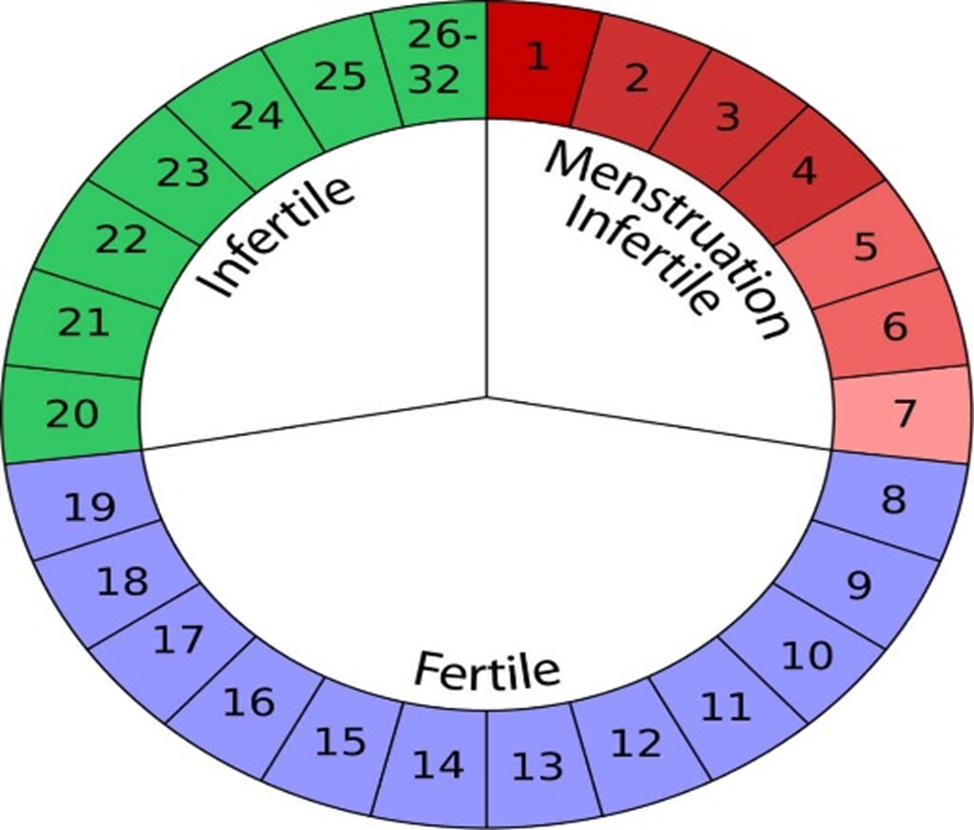
2). The calendar method (Safe period/rhythm method): The calendar method, also known as the rhythm method or safe period method, involves using a mathematical formula to estimate a woman’s fertile period. To use this method, a woman must first observe the length of her menstrual cycles for at least six months. The fertile period is calculated using the following formula: subtract 18 days from the shortest cycle to determine the first day of the fertile period, and subtract 11 days from the longest cycle to identify the last day of the fertile period. This method often requires a longer period of abstinence compared to other natural family planning methods, which contributes to its relatively high failure rate.
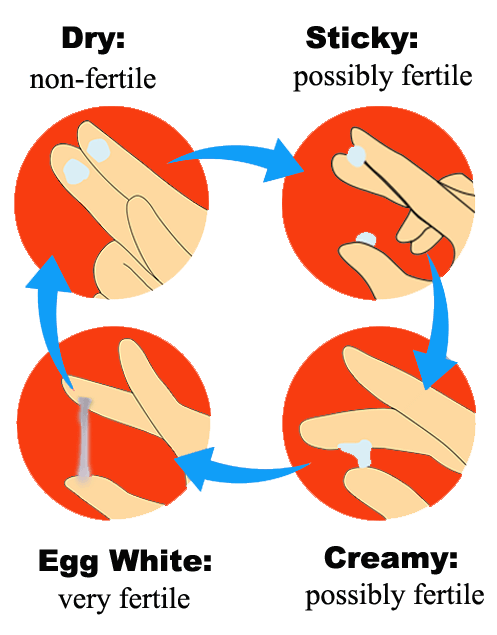
3). Cervical mucus method: The cervical mucus method involves monitoring the quality and quantity of cervical mucus at the vaginal opening to determine fertility. Fertile mucus, typically observed around mid-cycle, is abundant, thin, slippery, and elastic, resembling raw egg white. In contrast, infertile mucus is thick, sticky, and scant, appearing at the beginning and end of the cycle. To avoid conception, abstinence is practiced during the presence of fertile mucus and for three days after its disappearance.
4). Basal body temperature: The basal body temperature (BBT) method involves monitoring a woman’s resting body temperature daily to identify ovulation. Before ovulation, the body temperature remains slightly lower, and after ovulation, it rises slightly by an average of 0.3–0.5˚C. To use this method effectively, a woman should measure her temperature early in the morning before getting out of bed. If a slight rise in temperature is observed, it is advised to abstain from sexual activity for at least three days to prevent conception.

5) Male withdrawal/coitus interrupts: The withdrawal method, also known as coitus interruptus, involves removing the penis from the vagina before ejaculation to prevent sperm from entering the vaginal canal. Ejaculation must occur completely away from the vagina and the female partner’s external genitalia. A major disadvantage of this method is that pre-ejaculatory fluid may contain sperm, which can result in pregnancy, contributing to its high failure rate of approximately 75%.
II). Chemical Method:
- Spermicides: Spermicides are chemical agents designed to inactivate or kill sperm, helping to prevent pregnancy. They are available in various forms, including jelly, paste, foam tablets, and suppositories.
a. Foam tablets: In Nepal, the primary spermicidal product available is Kamal Chhaki (vaginal suppository). A woman inserts one Kamal Chhaki into the vagina 7–10 minutes before intercourse. The body heat melts the suppository, transforming it into a foam that acts as a barrier to sperm, providing contraceptive protection.
b. Jelly, paste and cream: These are vaginal contraceptive methods that a woman applies shortly before sexual intercourse. They act as spermicides, similar to suppositories, and are available in the form of jelly, paste, or cream. Using a special applicator, the product is inserted into the vagina 3–4 minutes before intercourse, creating a barrier that inactivates sperm and helps prevent pregnancy.
Mechanism of action
Spermicides work by inactivating sperm to prevent pregnancy. They are placed in the vagina to inactive sperm before they can pass through the cervix. While spermicides are somewhat effective when used alone, their effectiveness increases significantly when combined with other contraceptive methods, such as condoms.
Effectiveness
Spermicides are less effective than methods like Depo-provera, combined oral contraceptives (COCs), intrauterine devices (IUDs), Norplant, or voluntary sterilization. When used alone, the risk of pregnancy is relatively high compared to these more reliable contraceptive options.
Indications
Spermicide is suitable for:
- Women of all ages, including adolescents and women over 35.
- Couples who need a backup contraceptive method.
- Individuals or couples who engage in sexual activity frequently.
- Couples requiring a temporary contraceptive method, such as those awaiting the initiation of another method postpartum or post-abortion.
- Breastfeeding women who require contraception, as spermicide does not interfere with lactation.
Advantages
- Certain types of spermicides, such as foams and creams, provide immediate effectiveness upon application.
- They do not interfere with the natural flow of sexual intercourse.
- They are free from systemic side effects, making them a safe option for many users.
- Spermicides can be used as an effective backup method alongside other contraceptive options.
- They pose no significant health risks related to their use.
- They are easily accessible over-the-counter, without the need for a prescription.
- Their simplicity and ease of use make them a convenient contraceptive choice.
- No medical examination is required before using spermicides.
Disadvantages
- Spermicides have a relatively high user failure rate compared to other contraceptive methods.
- For certain forms like vaginal foaming tablets and suppositories, users must wait 7-10 minutes after insertion before engaging in intercourse.
- Spermicides need to be applied before each episode of intercourse, making them less convenient for some users.
- They are only effective for 1-2 hours, requiring reapplication for longer sessions.
- Couples may require counseling to ensure proper use and to address any concerns.
- Spermicides can be messy, which may interfere with sexual pleasure or comfort.
III). Mechanical methods
1. The diaphragm: The diaphragm is a flexible, dome-shaped latex or silicone barrier contraceptive designed to be inserted into the vagina to cover the cervix, preventing sperm from entering the uterus. It must be used with spermicide, which is applied inside the diaphragm before insertion to enhance its effectiveness. The diaphragm can be inserted up to 6 hours before intercourse and should remain in place for 6-8 hours after intercourse. It is important to not leave the diaphragm in for more than 24 hours to reduce the risk of infection.
This method is not as widely available in Nepal and requires a prescription and proper fitting from a healthcare provider. Regular check-ups are recommended to ensure the diaphragm fits correctly, especially after significant weight changes or childbirth. While the diaphragm can be an effective method of contraception when used correctly, its effectiveness depends on correct use, including proper insertion and the consistent use of spermicide.
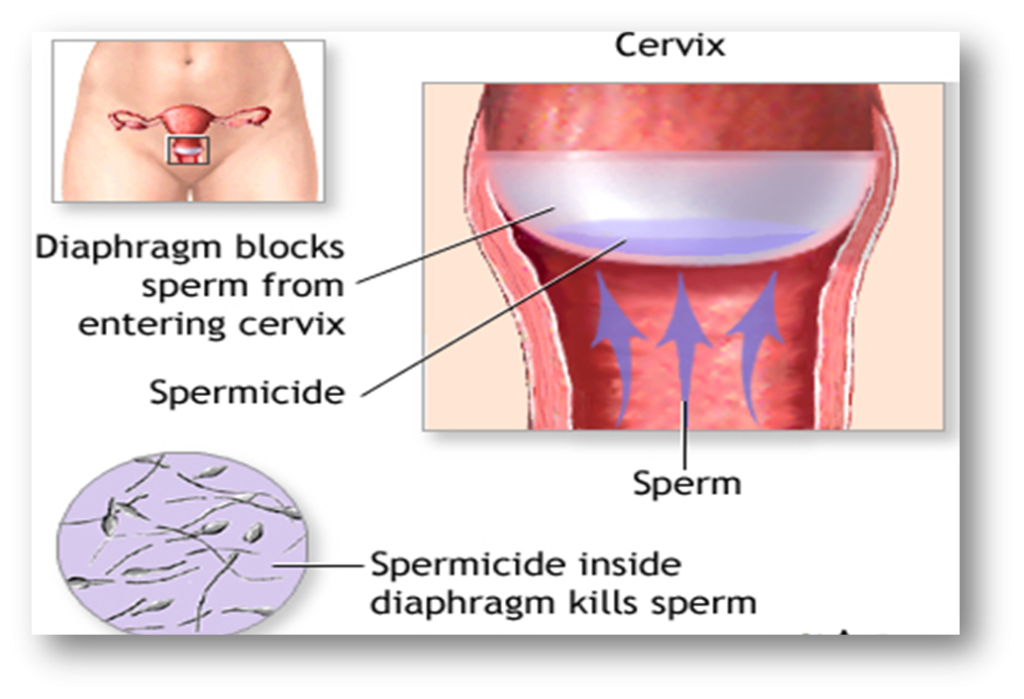
Mechanism of action
The diaphragm prevents sperm from entering the upper reproductive tract, including the uterus and fallopian tubes. It works in conjunction with spermicide, which it holds in place to immobilize and inactivate sperm.
Effectiveness
Diaphragms are less effective than condoms but provide greater effectiveness compared to using spermicides without any barrier.
Indications for use
- Couples aiming to space their pregnancies.
- Breastfeeding women who require contraception.
- Couples seeking a backup contraceptive method.
- Individuals who engage in frequent sexual activity or have multiple partners.
- Women who prefer to avoid hormonal contraceptive methods or are advised not to use them (e.g., smokers over the age of 35).
- Women who either do not want or cannot use intrauterine devices (IUDs).
Advantages
- Can be inserted up to 2 hours before sexual activity.
- Does not interfere with menstrual cycles.
- Has no impact on future fertility.
- Safe for use during breastfeeding.
- Provides immediate contraceptive effectiveness and is fully reversible.
- Can remain effective for a significant period when used correctly.
- When combined with spermicide, it reduces the risk of pelvic inflammatory disease. Offers protection against cervical cancer
Disadvantages
- Requires a trained professional for proper fitting.
- Can be challenging for some women to learn how to use it correctly.
- May cause vaginal irritation or increase the risk of urinary tract infections.
- Not recommended for women with uterine prolapse.
- Can be messy and might interfere with sexual pleasure.
- May cause allergic reactions in some individuals.
- Must be correctly placed each time a woman engages in vaginal intercourse.
2. Cervical cap: The cervical cap is smaller than a diaphragm and made of synthetic rubber. It is available in various sizes to suit individual needs. It should not be left inside the body for more than 3 days, as prolonged use may cause infection. After each use, it should be cleaned thoroughly and stored in a dry, safe place for reuse. It is not suitable for women with a prolapsed uterus.
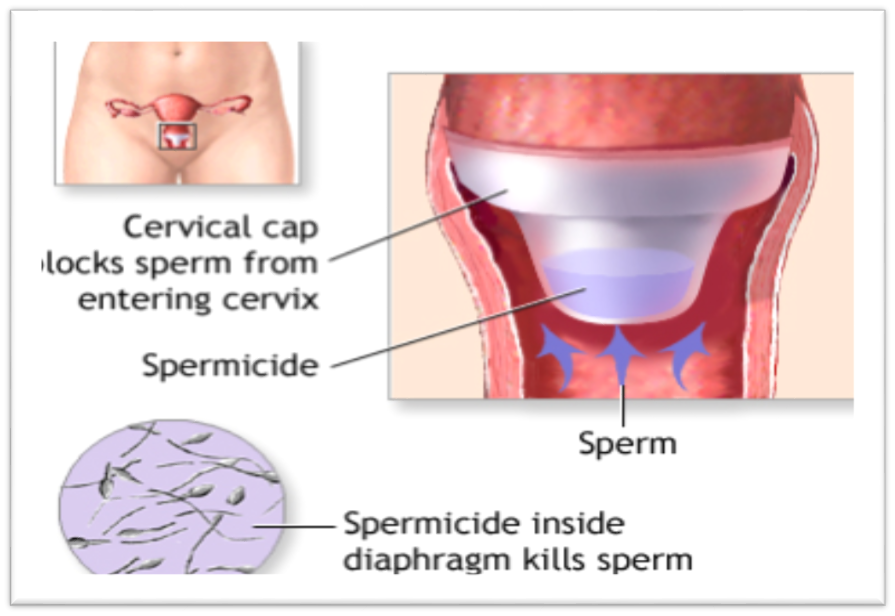
Mechanism of action
The cervical cap works by creating a barrier that prevents sperm from entering the uterus, as it fits securely over the cervix. To enhance its effectiveness, spermicide is applied to the cap before insertion. Once in place, the cap can remain in the vagina for up to 48 hours, offering protection during this time.
3. Condom
a). Male condom (Dhal):The male condom is the most commonly used contraceptive device for men. It is a thin, cylindrical sheath made of latex (rubber) that is worn over the erect penis during sexual intercourse. The open end of the condom has a thick rim, while the closed end may either be plain or feature a small reservoir (teat) to collect sperm.
In Nepal, condoms, commonly referred to as “Dhal,” are widely available and can be obtained free of charge from government and non-governmental family planning clinics. Condoms work by creating a physical barrier that prevents sperm from entering the vagina, thereby reducing the risk of pregnancy.
In addition to being an effective contraceptive method, condoms are highly effective in preventing the transmission of sexually transmitted diseases (STDs), including HIV/AIDS. This dual protection makes condoms an essential tool for promoting sexual and reproductive health.
Mechanism of Action
The male condom prevents sperm from entering the female reproductive tract, acting as a barrier to block fertilization. Additionally, it provides protection against the transmission of microorganisms, including sexually transmitted infections (STIs) such as gonorrhea, chlamydia, hepatitis B (HBV), and HIV/AIDS, by preventing direct contact between partners.
Effectiveness
When used correctly and consistently during every sexual encounter, condoms are highly effective in preventing pregnancy. The failure rate is approximately 2-5 pregnancies per 100 women per year when condoms are used properly. This emphasizes the importance of correct and consistent usage for optimal effectiveness.
Indications
- Men who wish to take an active role in family planning.
- Individuals who require contraception for occasional sexual activity.
- Couples who want to space their children but are open to having another child if it occurs.
- Couples seeking an immediate contraceptive option.
- Couples in need of a backup contraceptive method.
- Individuals concerned about the side effects of other contraceptive methods.
- People with multiple sexual partners.
- Men or women at risk of sexually transmitted infections (STIs), including HBV and HIV/AIDS.
- During the early postpartum period, particularly if breastfeeding, when fertility is naturally reduced.
Advantages
- Condoms offer immediate and reliable protection when used correctly.
- They do not pose any health risks related to the method itself.
- Condoms are inexpensive and easily accessible without a prescription.
- No medical examination or prescription is required for use.
- Condoms provide protection against HIV/AIDS, hepatitis B, sexually transmitted diseases (STDs), and can reduce the risk of infertility associated with some STIs.
- Easy to use and convenient for both partners.
- Condoms encourage male involvement by providing a way for men to take responsibility for contraception
- Can be used in conjunction with other forms of contraception for added protection.
- Some studies suggest that condom use may help lower the risk of cervical cancer.
- Particularly beneficial in the postpartum period, especially within the first 4 months after delivery.
- Condoms help reduce the risk of ectopic pregnancies by preventing fertilization.
Disadvantages
- Incorrect use or failure to use condoms consistently can lead to a higher rate of contraceptive failure.
- Condoms may reduce penis sensitivity, making it more challenging to maintain an erection during intercourse.
- Some male may feel embarrassed or self-conscious about using condoms, which can affect consistent use.
- A new condom must be used with each sexual encounter, which can be inconvenient.
- Proper disposal of used condoms can be a challenge, as they must be disposed of in a hygienic manner.
- Some individuals may be allergic to latex or other materials used in condoms, leading to discomfort or irritation.
How to use condom
- To use a condom, it should be rolled onto the erect penis before any sexual contact, as semen containing active sperm can be released even before ejaculation.
- If the condom lacks a reservoir tip, leave about 1-2 cm of space at the tip to collect the semen. After ejaculation, withdraw the penis while it is still erect, holding the base of the condom with fingers to prevent it from slipping off and to avoid spillage of semen.
- Each condom should be used only once and then discarded. Before discarding, tie a knot in the condom to prevent semen from spilling.
- Always keep an extra supply of condoms on hand, but ensure they are stored in a cool, dry place.
- Avoid storing condoms in warm or humid conditions, as this can cause them to deteriorate, making them more likely to break during use.
- Additionally, do not use lubricants such as mineral oil, cooking oils, or petroleum jelly (e.g., Vaseline) with condoms, as these substances can weaken the material and increase the risk of breakage.
b). Female condom: –The female condom is a strong, soft, and transparent polyurethane sheath measuring 17 cm (approximately 6.5 inches), similar in length to a male condom but wider. It features a flexible ring at each end. The inner ring aids insertion and secures the condom in place during sexual intercourse, while the softer outer ring remains outside the vagina. Designed to be inserted into the vagina before sexual activity, the female condom provides effective protection against pregnancy and sexually transmitted infections, including HIV/AIDS. It can be inserted up to 8 hours prior to sexual intercourse.

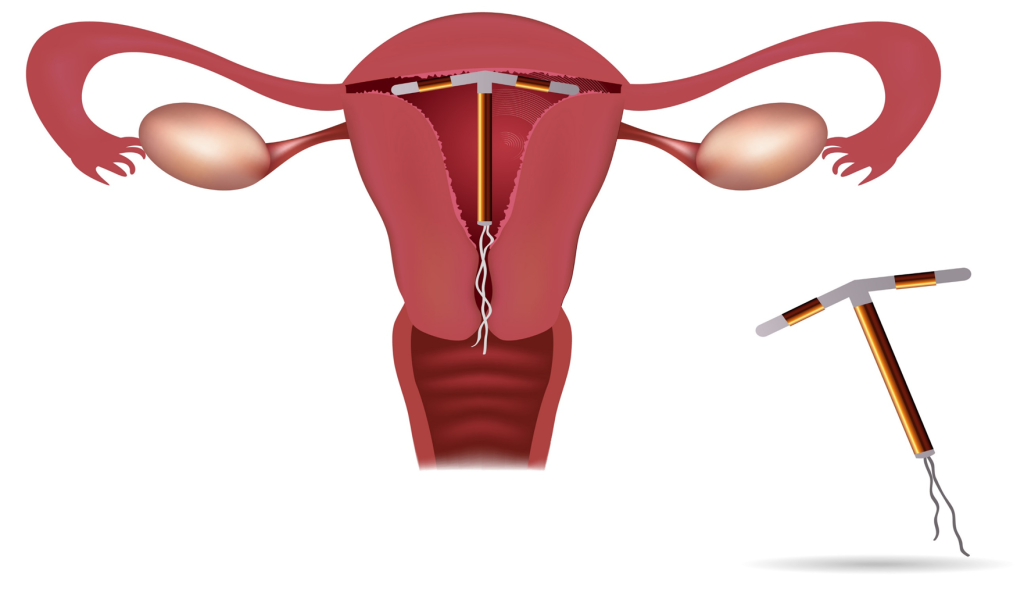
4. Intra Uterine Contraceptive Device (IUCD): The IUCD is one of the most widely used and safest methods of contraception available to women globally. The Copper T 380A, recently approved for use up to 12 years, is shaped like a “T.” It features a copper-coated stem and arms, providing a total exposed copper area of 380 square millimeters.
The device includes white or blue strings that extend through the cervical opening into the vagina, allowing for easy removal. The Copper T branch is positioned at the base of the uterus during placement. Currently, it is estimated that over 100 million women use IUCDs worldwide.
Types of IUCDs
Intrauterine Contraceptive Devices (IUCDs) are categorized into three generations based on their composition and mechanism of action:
1. Non-medicated IUCDs (1st Generation): These devices represent the earliest form of intrauterine contraception. Made from materials such as polyethylene or polymers, they do not contain any active substances. They function primarily by creating a physical barrier within the uterus to prevent fertilization or implantation. Examples: Loops, spirals, coils, rings.
2. Medicated IUCDs (2nd Generation): The second-generation IUCDs incorporate copper as the active component. Metallic copper has strong anti-fertility properties, which include reducing sperm motility, viability, and altering the uterine environment to prevent implantation. These devices are highly effective and are widely used due to their long-lasting contraceptive protection. Examples:
- Copper-7: A curved device designed for easy insertion.
- Copper T-200: A T-shaped device with copper along the stem and arms.
- Copper T-380A: A T-shaped device with a total copper surface area of 380 square millimeters, providing up to 12 years of protection.
3. Hormone-Releasing IUCDs (3rd Generation): Hormonal IUCDs release small amounts of hormones, typically progesterone or its synthetic derivatives, directly into the uterus. These hormones work by thickening cervical mucus to block sperm, inhibiting ovulation, and altering the uterine lining to prevent implantation. They also help in reducing menstrual bleeding and cramping. Examples:
- Progesterone-releasing devices: Release hormones gradually at a controlled rate, such as 65 mcg per day.
- Levonorgestrel-releasing devices (e.g., Mirena): Widely used for both contraception and therapeutic benefits, such as treating heavy menstrual bleeding or endometriosis
Mechanism of action
Copper-releasing intrauterine devices (IUDs) work by releasing copper ions, which interfere with sperm motility and survival, altering cervical mucus to prevent sperm from reaching the cervix. Copper also enhances the cellular response in the endometrium and affects uterine enzymes, making the environment unfavorable for implantation. Progestin-releasing IUDs, on the other hand, thicken cervical mucus to block sperm entry, maintain high progesterone levels in the endometrium, and lower estrogen levels, further altering the endometrium to prevent implantation.
Effectiveness
The intrauterine contraceptive device (IUCD) is highly effective, with a success rate of 99.2%
Timing of insertion
- The intrauterine contraceptive device (IUCD) can be inserted at any time during the menstrual cycle, provided it is certain that the woman is not pregnant.
- The best time for IUCD insertion is within the first 1-7 days of the menstrual cycle.
- After childbirth, the IUCD can be inserted within 6 weeks postpartum.
- If the woman is using lactational amenorrhea (LAM) as contraception, the IUCD can be inserted after 6 months postpartum.
- Following an abortion, the IUCD can be inserted immediately or within 7 days, provided there is no evidence of pelvic infection.
Indications
- Women of any reproductive age.
- Postpartum women who are not breastfeeding.
- Women following an abortion, with no contraindications.
- Women at low risk for genital tract infections (GTIs) and sexually transmitted infections (STIs), such as HBV and AIDS.
- Women who prefer not to or should not use hormonal contraceptive methods.
- Women who have difficulty remembering to take a daily pill.
- Breastfeeding mothers in need of contraception.
- Women who want a highly effective, long-lasting contraceptive but are not ready for a permanent method.
- Women who prefer to avoid hormonal contraceptives or have health reasons to do so, such as smokers over 40 years old who smoke more than 15 cigarettes a day.
Contraindications
- IUCD should not be used if the woman is pregnant.
- Acute Pelvic Inflammatory Disease (PID) or a history of PID.
- Sexually Transmitted Diseases (STDs), including lower genital tract infections.
- High risk of STDs due to multiple sexual partners of the woman or her partner.
- Known or suspected malignancy of the genital tract, including cases of undiagnosed dysfunctional uterine bleeding.
- Congenital abnormalities of the uterus.
- Untreated acute cervicitis, including bacterial vaginosis, until the infection is controlled.
- Conditions associated with an increased susceptibility to infections caused by microorganisms.
Advantages
- Highly effective, immediate, and cost-efficient contraceptive method.
- Does not interfere with sexual intercourse.
- Associated with minimal side effects.
- Provides long-term effectiveness, lasting up to 12 years.
- Suitable for breastfeeding women.
- Appropriate for women of any age group.
- Follow-up services are available to address any problems.
- High rate of continuation among users.
Disadvantages
- A pelvic examination and screening are required before insertion.
- Insertion and removal must be performed by a trained healthcare professional.
- The device may be spontaneously expelled.
- It does not provide protection against STDs, AIDS, or HIV.
- Menstrual bleeding and cramping may increase during the first few months of use.
- The client cannot remove the device on their own.
- There is an increased risk of pelvic inflammatory disease (PID) for individuals with a recent history of STDs or those with multiple sex partners.
Side effects and problems
- Bleeding or spotting between periods
- Missed or late periods
- Heavy or prolonged periods
- Painful periods, which may lead to anemia
- Vaginal discharge or suspected pelvic inflammatory disease (PID)
- Pain or cramps during or following insertion
- Backache or allergic skin reactions due to copper (in the case of Copper T)
Follow up care
Clients should return to their IUD provider after the first post-insertion menses (4-6 weeks) but no later than 3 months for their first check-up. They should be strongly encouraged to visit their provider anytime they experience any problems. The routine follow-up schedule is as follows:
- First : After 1 week
- Second : After 1 month or after the first menses
- Third : After 2 months
- Fourth : After 6 months
- Fifth : After 12 months
Post IUD client instruction
The client should regularly check the strings after each menstrual period.
- Wash hands thoroughly before checking the strings.
- Sit in a squatting position or place one foot on a step or ledge for easier access.
- Insert the middle or second finger into the vagina to locate the opening to the uterus. The cervix will feel firm, similar to the tip of the nose.
- Feel for the strings. If the strings are felt, it indicates that the IUD is correctly in place.
- Never pull on the strings, as this could cause the IUD to be expelled or potentially damage the cervix.
- If the client cannot feel the strings, or if they feel longer or shorter than usual, she should consult the IUD provider and refrain from having sex until the IUD is replaced.
- Most expulsions occur during menstruation, so the IUD user should check their menstrual pads for any signs of expulsion. If the device is accidentally expelled, the client should return to the IUD provider for the possible insertion of a new IUD.
Common complications
- Bleeding and lower abdominal pain.
- Menstrual changes such as heavier bleeding, intermenstrual bleeding, or spotting are normal in the initial months. Clients should be reassured that these changes are expected and typically resolve after a few months.
Warning/danger signs for IUDs
A woman should seek medical help as soon as possible if she experiences any of the following problems:
- P: Periods are late, or there is abnormal spotting or bleeding.
- A: Abdominal pain, pain during intercourse, or severe cramping.
- I: Exposure to infection, or abnormal vaginal discharge.
- N: Not feeling well, fever, chills, especially when accompanied by lower abdominal pain.
- S: Missing strings, or if the strings feel shorter or longer than usual, or if the plastic tip of the IUD cannot be felt when checking the strings.
IV). Hormonal methods or physiological method
Oral contraceptive pills, commonly known as birth control pills, are a method of preventing pregnancy by using hormones to stop the ovaries from releasing eggs.
There are two main types of oral contraceptive pills:
- Progestogen only pill (Mini Pill): Contains only one hormone, progestogen, which alters the cervical mucus to prevent sperm from reaching the uterus.
- Combined Pill: Contains both estrogen and progestin, which work together to stop ovulation and modify the uterine lining to prevent pregnancy.
1.Combined Oral Contraceptives (COCs): Combined oral contraceptive pills are considered a very reliable method of contraception. All combined COCs contain two hormones: estrogen and progesterone. Estrogen in the pills typically prevents the release of eggs from the ovaries (ovulation). Progesterone causes the cervical mucus to become thick and scanty, which prevents sperm from traveling into the uterus, thus reducing the likelihood of fertilization.


Types of combined oral contraceptives (COCs) in Nepal
In Nepal, the most common COCs are low-dose pills in a 28-day package. Some of the widely used options include:
- Gulaf: Contains 50 mcg of Menstranel (estrogen) and 1 mg of Norethindrone (progesterone). The brownish tablet also contains 75 mg of ferrous sulfate.
- Nilocan: Contains 35 mcg of Ethinyl Estradiol (estrogen) and 0.5 mg of Norethindrone (progesterone). This pill has a lower progesterone content, resulting in fewer side effects.
- Lo-Femenal: It contains 0.3 mg of Norgestrel (progestin) and 0.03 mg of Ethinyl Estradiol (estrogen) in each pill. The last 7 brown placebo pills contain 75 mg of ferrous sulfate (iron).
- Sequential estrogen: Taken alone for 14-16 days, starting on the 5th day of the menstrual cycle, followed by a combination tablet containing both estrogen and progesterone for the next 5-7 days.
- Micro Pills (Progesterone only): These are low-dose pills taken for 30 days, including during menstruation. A small dose of progesterone does not interfere with pituitary-hypothalamic-ovarian functions.
Mechanism of action
Combined Oral Contraceptives (COCs) prevent pregnancy through multiple mechanisms of action. Firstly, they suppress ovulation, inhibiting the release of eggs from the ovaries. Additionally, they reduce sperm transport within the upper genital tract, including the fallopian tubes, thereby decreasing the likelihood of sperm meeting the egg. COCs also alter the endometrial lining, making it less suitable for implantation if fertilization occurs. Furthermore, they thicken cervical mucus, creating a barrier that prevents sperm from penetrating the cervix and reaching the egg. These combined effects make COCs an effective method of contraception.
Effectiveness
COCs are 99.9% effective in preventing pregnancy when used correctly. This high effectiveness rate is achieved when the pills are taken consistently and as directed, without missing any doses.
Indications
- Have irregular menstrual cycles.
- Experience severe menstrual cramping.
- Have anemia due to heavy menstrual bleeding.
- Seek a highly effective method of contraception.
- Complain of menstrual cycle-related symptoms, such as mid-cycle ovarian pain or premenstrual syndrome (PMS).
Contraindications
Absolute contraindications
- Severe hypertension
- Venous thrombosis (blood clots)
- History of cholestatic jaundice during pregnancy
- Confirmed pregnancy
- Undiagnosed vaginal bleeding
Relative contraindication
- Obesity
- Varicosities (vein problems)
- Epilepsy
- Depression and mood fluctuations
- Age over 35 years
- Smoking more than 15 cigarettes per day
- Breastfeeding mothers less than 6 months postpartum
When to start COCs
- When it is reasonable to believe the client is not pregnant and there has been no intercourse since the last normal menses.
- After the correct and consistent use of a reliable contraceptive method.
- Within 6 weeks postpartum for non-breastfeeding women.
- Within 4 months postpartum for breastfeeding women.
- Within the first 5 days of menstruation, post-abortion, or immediately after childbirth.
Advantages
- Highly effective, provides 99.9% effectiveness when used correctly.
- Few health risks associated with minimal method-related health risks.
- Simple and easy to use.
- Easily available for free at health facilities or at low cost from medical shops.
- Makes menstrual cycles regular and alleviates dysmenorrhea.
- Prevents anemia, reduces blood loss during menstruation and provides ferrous sulfate.
- Reduces the chances of developing cancers of reproductive organs and pelvic inflammatory disease.
Disadvantages
- Requires daily intake; forgetfulness can lead to failure.
- Certain medications, such as rifampicin and phenytoin, may interact with COCs, reducing their effectiveness.
- Does not provide protection against sexually transmitted diseases (STDs), including HIV/AIDS and HBV.
- Minor side effects may include:
- Nausea
- Amenorrhea
- Breast tenderness
- Spotting or breakthrough bleeding between periods
- Headaches
- Weight gain
- Mood changes
- Dizziness
- Fluid retention, potentially causing high blood pressure in some women
- Decreased milk production during breastfeeding
Client instructions for taking COC
- How to take the pills:
- Take one pill each day at the same time of the day, preferably at bedtime.
- Start taking pills within the first 5 days of your menstrual cycle to ensure maximum effectiveness.
- Following the pack:
- Begin with the pill in the top left-hand corner of the packet.
- Follow the direction indicated by the arrows on the pack.
- Take the white pills daily for 21 days (active pills).
- Then, take the brown pills daily for 7 days (placebo pills) until the packet is finished.
- Side effects to expect:
- During the first one or two packs, you may experience:
- Bleeding between periods
- Nausea
- Dizziness
- Headaches
- These symptoms are not dangerous and typically subside after one or two cycles.
- During the first one or two packs, you may experience:
- When to return to the clinic:
- If discomfort persists or becomes severe, visit the clinic for advice and support.
- Starting a new packet:
- When the 28-day packet is finished, begin a new packet the very next day without missing any days.
Instructions for missed pills
- Missing one or more pills may lead to breakthrough bleeding or spotting, and more importantly, an increased risk of pregnancy.
- If one pill is missed take the missed pill as soon as possible, even if it means taking two pills on the same day (the missed pill and the regular pill).
- If two or more pills are missed take two pills each day until you catch up. Use a condom or avoid having sex for the next 7 days to ensure protection.
- If you often forget to take your pills or interrupt your pill schedule, consult the clinic staff about switching to another family planning method that suits your lifestyle better.
Instructions for missed menstrual period
- If she misses two or more menstrual periods, she should consult a healthcare provider to rule out pregnancy.
Pills and medical care
- She should bring the pill packet with her to each return visit. Clinics typically supply pills for up to three months at a time.
- It’s important for her to mention that she is taking pills whenever visiting a healthcare provider.
Risks of exposure to STDs, Including HIV/AIDS
- She should use condoms in addition to the pills if she believes there is any risk of exposure to sexually transmitted diseases (STDs), including HIV/AIDS, as the pills do not offer protection against infections.
Backup method
- If she starts taking the pills more than 5 days after the start of her menstrual cycle, she should use condoms for the next 7 days to ensure effectiveness.
- In case of severe vomiting or diarrhea, combined oral contraceptives (COCs) may not work effectively. She should use condoms or refrain from sex until she is well and has taken the white pills for 7 consecutive days.
Return and Follow-up visit
- The first follow-up visit should be scheduled 3 months after starting the pills.
2. DMPA/Depo-Provera
Injectable contraceptives, such as Depo-Provera, contain only the hormone progestin and were developed in the 1950s. Initially, they were used to treat conditions like endometriosis, endometrial cancer, dysmenorrhea, hirsutism, and bleeding disorders. By the 1960s, they were adopted as a form of contraception. The progestin in DMPA works by suppressing ovulation, meaning it prevents the release of mature eggs from the ovaries, effectively preventing pregnancy.
Injectable contraceptives like Depo-Provera contain only the hormone progestin. Developed in the 1950s, they were initially used to treat conditions such as endometriosis, endometrial cancer, dysmenorrhea, hirsutism, and bleeding disorders. By the 1960s, these injections became widely used as contraceptives. The progestin in DMPA works by suppressing ovulation, meaning it prevents the release of mature eggs from the ovaries. Additionally, it thickens the cervical mucus, making it difficult for sperm to penetrate the cervix.
The only injectable contraceptive available in Nepal is Depot-Medroxy Progesterone Acetate (DMPA). The brand name is Depo-Provera, commonly referred to as Depo. CRS Company distributes it under the name “Sangini” or “Teen Mahiney Sui.” DMPA comes in a single-dose vial containing 150mg (1ml) for a three-month period and is administered intramuscularly.

Mechanism of action
- DMPA prevents ovulation by suppressing the mid-cycle LH peak, which is essential for egg release from the ovaries.
- The hormone thickens and makes the cervical mucus more viscous, which prevents sperm from penetrating the cervix and reaching the egg.
- The endometrium becomes atrophic (thin), reducing the likelihood of implantation. This results in lighter menstrual bleeding or, in some cases, the cessation of menstruation for several months.
Effectiveness
Depo-Provera is one of the most effective temporary family planning methods, with a failure rate of less than 1%. It has been shown to be even more effective than combined oral contraceptives (COCs).
Indications
- Suitable for healthy women who are seeking contraception.
- Ideal for women who want long-term spacing between pregnancies.
- Suitable for those who prefer a contraceptive method that does not require daily action or action before intercourse (unlike barrier methods).
- Recommended for women who cannot use contraceptives containing estrogen.
- Safe for breastfeeding women after 6 weeks postpartum, providing effective contraception.
- A good option for women who are heavy smokers (more than 15 cigarettes daily) or have hypertension and cannot use combined oral contraceptives (COCs).
- Useful for women who want a temporary method while they or their partner are awaiting permanent sterilization.
Contraindications
- Any unexplained vaginal bleeding should be investigated before using Depo-Provera.
- Should not be used if pregnancy is suspected or confirmed.
- Women with a history of ectopic pregnancy may face increased risks with Depo-Provera.
- Women who experienced pruritis (itching) during a previous pregnancy should avoid this method.
- Women with a history of herpes or unexplained jaundice should not use Depo-Provera.
- Women with severe liver impairment or liver diseases such as hepatic adenoma.
- Women with a history of thrombo-embolic disorders or those with high risk for arterial disease.
- Contraindicated in women with breast cancer (current or history of).
- Should not be used after the evacuation of a hydatidiform mole (a non-viable pregnancy).
- After a missed or incomplete abortion until fully resolved.
Advantages
- Over 99% effective at preventing pregnancy when used correctly.
- Provides immediate contraception if given during the first 5 days of the menstrual cycle.
- Convenient for the user, as the mother can choose this method with minimal hassle.
- Offers long-term contraception, with an injection every 3 months.
- A pelvic exam is not needed to start Depo-Provera use.
- There are fewer method-related health risks since Depo-Provera does not contain estrogen.
- Does not interfere with sexual desire or enjoyment.
- Requires only one injection every 3 months, and no daily or pre-intercourse action is needed.
- Clients do not need to keep additional supplies, as the injection is administered at the healthcare provider’s office.
- Contraceptive effectiveness remains intact even if the client is up to 2 weeks late for her return visit.
- Depo-Provera does not adversely affect breastfeeding, making it safe for postpartum women.
- Fertility returns after discontinuation of the method, making it a reversible contraception option.
- Depo-Provera can be easily administered by a non-physician, such as a nurse or other trained healthcare provider.
- Depo-Provera can be used safely by women over 40, offering flexibility in contraception for this age group.
- Suitable for women who do not wish to have more children but prefer not to undergo permanent sterilization.
- Can be used by women who are post-abortion, offering a safe and effective contraceptive option during recovery.
Disadvantages
- Depo-Provera does not protect against most sexually transmitted infections (STIs), including HIV/AIDS. Additional barrier methods, like condoms, are recommended for STI protection.
- Most users experience menstrual changes, such as irregular bleeding or spotting. About 50-80% of users may experience amenorrhea (absence of menstruation) after using Depo-Provera.
- There may be a delay in the return of fertility after discontinuing the method, which can take several months.
- Users must return to the health post or attend a mobile outreach clinic for injections, which may be inconvenient for some.
- The client cannot discontinue the method on her own before the next injection. She must wait until the next scheduled appointment.
- Weight gain is a common side effect associated with Depo-Provera use.
- Some users may experience mood changes, including depression, while using this contraceptive.
Timing of DMPA Injection
DMPA can be given at any time during the menstrual cycle, as long as it is confirmed that the client is not pregnant.
- Optimal timing for the first injection
- During menstruation: The optimal time for the first injection is between the 5th and 7th day of menstruation.
- Post-abortion: The injection can be given immediately after an abortion or within 7 days.
- Postpartum: For postpartum mothers, DMPA can be administered when the mother brings her infant for immunization, typically around 6 weeks postpartum.
- Exclusive breastfeeding: If the mother is exclusively breastfeeding and has not yet started menstruating, the DMPA injection can be delayed up to 6 months postpartum.
Side effects
- Prolonged bleeding during menstruation.
- Unexpected bleeding or spotting between periods.
- Around 5% of users may experience amenorrhea at all after one year of use.
- A slight increase or decrease in weight, typically within 2 kg.
- Breast tenderness or discomfort.
Other side effects
- Headaches, nervousness, depression, mental changes
- Abdominal discomfort and swelling
- Gastrointestinal disturbances
- Limb pain and varicose vein pain
- Nausea and vomiting
- Changes in or loss of libido
- Dizziness or fainting
- Vaginal discharge or breast discomfort
- Dysmenorrhea (painful periods)
- Severe cramping or pain during menstruation.
- Hair or skin changes
- Hair loss
- Hirsutism, excessive growth of hair (e.g., on the face, chest, and back) in women.
- Chloasma, a condition where brown or gray-brown patches appear on the skin, usually on the face.
- Intertrigo, a skin fold rash caused by heat, moisture, and friction, common under breasts, in the groin, and abdominal folds.
- Allergic skin rashes or pruritis of the skin.
Warning signs
The warning signs of DMPA include excessive weight gain, severe headaches, heavy bleeding, depression, and frequent urination. If any of these symptoms occur, it’s important to consult a healthcare provider for proper assessment and guidance.
Client’s Instructions
- Additional injections: Instruct the client to return to the health center for the next DMPA injection every 3 months. The next injection can be given from 2 weeks before or 2 weeks after the 12-week interval is completed.
- Medical concerns: The client should return to the clinic if any medical issues arise, such as heavy vaginal bleeding, prolonged bleeding, delayed menstrual periods, or any other concerns.
- Side effects: Explain the possible side effects of DMPA and provide guidance on what to do if they occur. Emphasize the importance of safe, effective, and continued use of the method.
- Follow-up: Instruct the client to return after 12 weeks for the next injection, but the injection can be administered 2 weeks before or 2 weeks after the appointment date (i.e., up to 10 weeks after the last injection).
3. Norplant
Norplant, a registered trademark of the Population Council, refers to subdermal implants, a new generation of long-acting contraceptives. This highly effective, reversible contraceptive method contains levonorgestrel, a progesterone hormone, which provides protection from pregnancy for up to seven years.
Previously, Norplant consisted of six capsules, each 34 mm long and 2.4 mm in diameter. Now, the Norplant implant is available as two flexible, scaled, white or off-white rods, each approximately 43 mm in length and 2.5 mm in diameter, to be inserted subdermally in the upper arm. Each implant contains 75 mg of levonorgestrel. The release rate of levonorgestrel is about 100 micrograms per day one month after insertion, declining to approximately 40 micrograms per day within one year, 30 micrograms per day within three years, and 25 micrograms per day within five years.
Mechanism of action
Norplant involves the inhibition of ovulation, thickening of cervical mucus to prevent sperm penetration into the uterus, and alteration of the endometrium, which reduces the likelihood of implantation. Additionally, it suppresses progesterone during the luteal phase, further contributing to its contraceptive effects.
Effectiveness
The average annual pregnancy rate is less than 1%.
Duration
- Indoplant: Effective for 3 years.
- JADELLE: Effective for 5 years.
Indications
- Healthy women seeking long-term spacing (i.e., 7 years).
- Women requiring immediate post-abortal contraception.
- Women who cannot use contraceptives containing estrogen.
- Women for whom an intrauterine contraceptive device (IUCD) is not ideal.
- Breastfeeding women who need a contraceptive.
- Women who prefer methods that do not require daily use or use before intercourse.
Contraindications
- Known or suspected pregnancy.
- Acute liver disease.
- Unexplained vaginal bleeding.
- Sickle cell anemia.
- Coronary artery or cardiovascular disease.
- High blood pressure.
- Thrombophlebitis.
Timing of insertion: Norplant can be inserted at any time during the menstrual cycle as long as the client is not pregnant.
Optimal times for insertion
- During menstruation: within 7 days from the onset.
- Post-abortion: immediately or within the first 7 days.
- Postpartum: at the time of the infant’s immunization (approximately 6 weeks).
- If exclusively breastfeeding and not menstruating, insertion can be delayed up to 6 months postpartum.
- If insertion occurs after 7 days of the menstrual cycle and no contraception has been used, a backup method (e.g., condoms) should be used for at least 7 days, especially if the client is in the mid-cycle or unsafe period.
Return of fertility: Fertility returns almost immediately upon removal of the implant capsules, without delay.
Choice for discontinuation: If a woman wishes to become pregnant, experiences side effects, or wants to switch to another contraceptive method, the implant capsules can be removed at any time. Removal should only be performed at a healthcare facility by trained professionals.
Advantages
- Highly effective.
- Provides long-term protection for up to 5 years.
- Immediate return of fertility after removal.
- No pelvic exam required.
- Safe, easy to use, and does not interfere with intercourse.
- Comfortable and unobtrusive.
- Can be used by post-abortion clients.
- Can be removed at any time.
- Offers continuous protection.
- Does not interfere with breastfeeding.
- Few method-related health risks as it contains no estrogen.
Disadvantages
- Does not protect against most STDs, including HIV/AIDS.
- Causes menstrual changes in most users, such as:
- Irregular bleeding or spotting.
- Prolonged or heavy vaginal bleeding.
- Amenorrhea (absence of menstruation) in 20% of users.
- Requires a minor surgical procedure for insertion and removal.
- Weight gain or loss may occur.
B. Permanent family planning/voluntary sterilization
Voluntary sterilization is a surgical procedure designed to permanently stop an individual’s ability to reproduce, applicable to both males and females. It is a highly effective and widely used method of long-term contraception, offering safety and minimal side effects.
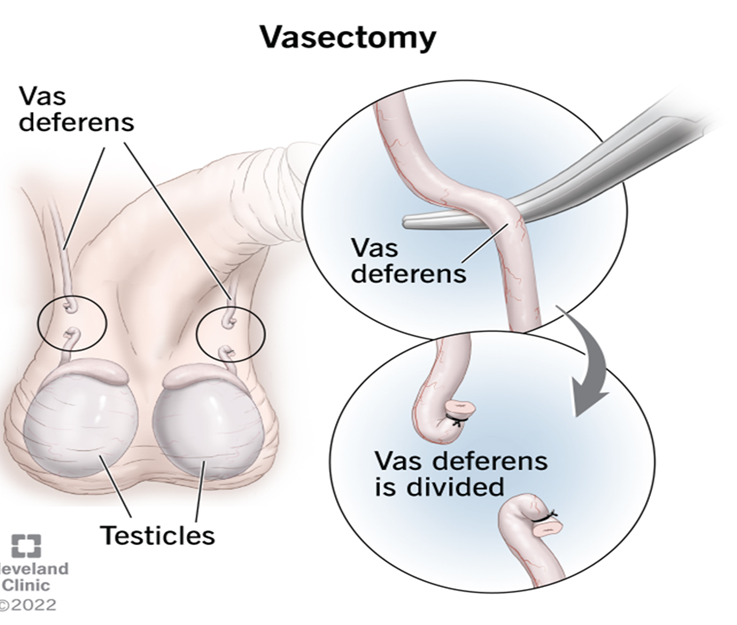
- Vasectomy
Vasectomy, a male sterilization procedure, is performed under local anesthesia. In this operation, the surgeon cuts and ties the vas deferens, the tubes that transport sperm from the testes to the penis. Following this minor surgery, sperm can no longer travel beyond the ends of the tubes.
Mechanism of Action
Vasectomy involves blocking the vas deferens, which prevents sperm from entering the semen. This ensures that fertilization cannot take place during sexual intercourse.
Types of Vasectomy
- Conventional Vasectomy: A surgical procedure involving small incisions on each side of the scrotum. The vas deferens is cut and sealed to prevent sperm from mixing with semen.
- No-Scalpel Vasectomy: A less invasive method where a tiny puncture is made in the scrotum using a special instrument. The same instrument is used to stretch the opening, allowing access to the vas deferens.
Effectiveness
- Failure rate: Less than 1%.
Timing of the procedure
Healthy males with no contraindications can undergo surgery at their convenience.
Indications
- Men of reproductive age, usually under 50, seeking permanent contraception.
- Men whose partners have health risks associated with pregnancy.
- Couples who have achieved their desired family size.
- Men providing informed and voluntary consent.
Contraindications
- Large varicocele
- Hydrocele
- Infection
- Diabetes
- Coronary heart disease
- Inguinal hernia
- Filariasis
- Atrophic or painful testes
- Scar tissue
- Previous scrotal surgery
- Tumors (benign or malignant)
Advantages
- Highly effective and permanent.
- Simple surgery with local anesthesia.
- Fewer surgical risks compared to female sterilization.
- No long-term side effects or expenses.
- Does not interfere with sexual function or intercourse
Disadvantages
- Permanent and difficult to reverse.
- Not immediately effective; requires up to 20 ejaculations to clear sperm.
- No protection against STDs or HIV/AIDS.
- Minor surgical risks.
- Potential regret in some cases.
Failure of Vasectomy
- Pregnancy may occur if contraceptives are not used during the first 3 months or 20 ejaculations after the procedure.
Client Instructions
- Pre-Operation
- Bathe and wear clean, loose-fitting clothes.
- Trim pubic hair to avoid obstruction during surgery.
- Bring clean scrotal support clothing.
- Post-Operation
- Rest for 2 days and wear scrotal support.
- Take analgesics (e.g., ibuprofen or paracetamol) for pain and swelling.
- Avoid heavy lifting, cycling, or sexual activity for 3 days to 1 week.
- Use condoms or alternative contraception for 3 months.
- Return for a semen test 3 months after surgery to confirm effectiveness.
Complications
- Surgical: Hematoma or infection.
- Spontaneous Recanalization: Rare cases where the vas deferens reconnects.
- Psychological: Complaints of reduced sexual vigor, impotence, headache, fatigue, etc.
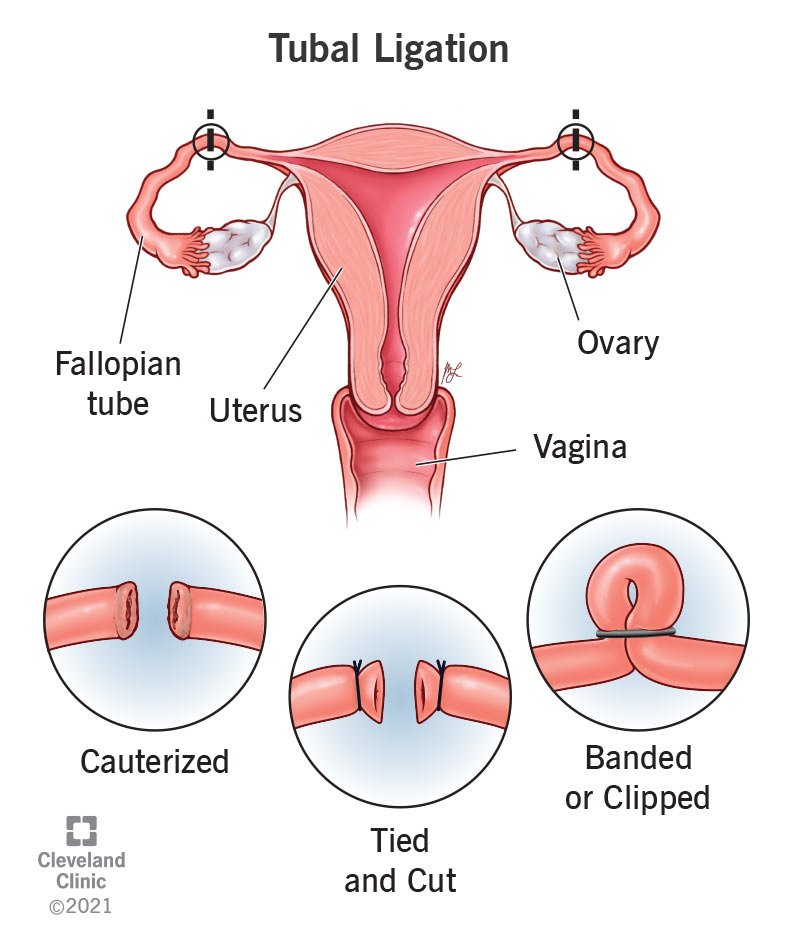
2. Female voluntary sterilization
It is a surgical procedure for permanently termination fertility in women called tubal ligation. The surgical approaches most often used: −
- Minilaparotomy involves making a small incision in the abdomen. The fallopian tubes are brought to the incision to be cut or blocked.
- Laparoscopy involves inserting a long thin tube with a lens in it into the abdomen through a small incision. This laparoscope enables the doctor to see and block or cut the fallopian tubes in the abdomen.
Mechanism of Action
Tubectomy prevents pregnancy by mechanically blocking the fallopian tubes through cutting or sealing them, thereby stopping the sperm from reaching the egg (ovum).
Effectiveness
Tubectomy is more than 99% effective in preventing pregnancy.
Indications
Tubectomy is suitable for:
- Women seeking highly effective and permanent protection against pregnancy.
- Women for whom pregnancy poses a serious health risk.
- Women who do not desire more children.
- Women who understand and voluntarily consent to the procedure.
- Women who do not prefer temporary contraceptive methods.
Contraindications
Tubectomy is contraindicated in women with the following conditions:
- Pregnancy
- Severe anemia
- Uncontrolled diabetes
- Heart disease
- High blood pressure
Timing of the procedure
- Postpartum: 6–8 weeks after delivery when pregnancy can be ruled out.
- During the menstrual cycle: At any time if pregnancy is confidently excluded.
- Mini-laparotomy: Should be performed within 48 hours of normal delivery.
- Age consideration: Women over 35 years may also opt for the procedure with appropriate counseling.
Advantages
- Highly effective and permanent.
- Simple surgical procedure, usually performed under local anesthesia.
- Requires no ongoing contraceptive management.
- Does not interfere with sexual activity.
- Immediate contraceptive effect post-procedure.
Disadvantages
- Irreversible and difficult to reverse.
- No protection against sexually transmitted diseases (STDs), including HIV/AIDS and hepatitis B.
- Risks associated with surgery, such as bleeding and infection.
- A small scar may be visible post-procedure.
Client Instructions
Before surgery:
- Bathe before arriving for the procedure.
- Prepare the surgical site by cleaning and shaving the area.
After surgery:
- Keep the incision site clean and dry for the first two days.
- Gradually resume normal activities as you feel better, but avoid heavy lifting or tension on the incision site for at least one week.
- Avoid sexual intercourse for at least one week or longer if discomfort persists.
- Contact the clinic if any of the following occur:
- Fever above 38°C (100.4°F).
- Dizziness or fainting.
- Persistent or increasing abdominal pain.
- Bleeding or fluid discharge from the incision site.
Pain management:
- For pain relief, take one or two tablets of ibuprofen or paracetamol as needed.
Dietary Instructions:
- Resume a normal diet. In case of abdominal discomfort, start with easily digestible foods.
Complications of tubectomy
- Bleeding during or after the procedure.
- Infection at the surgical site.
- Damage to the bladder.
- Perforation of the uterus.
- If pregnancy occurs after tubectomy, there is a higher risk of ectopic pregnancy (a pregnancy developing in the fallopian tubes).
Unmet need for Family Planning
Definition
Unmet need for family planning refers to the gap between women who want to avoid or delay pregnancy and those who are not using any effective contraceptive method. This includes women who are sexually active, fertile, and want to stop or delay childbearing but are not using modern contraception.
Global unmet need for contraception
Globally, approximately 214 million women of reproductive age in developing regions who wished to avoid pregnancy were not using modern contraceptive methods (Guttmacher Institute, 2017). This figure represents a decrease from 225 million in 2014, showing some progress in addressing the unmet need for contraception. However, as of 2021, an estimated 164 million women worldwide still had an unmet need for family planning, underscoring the persistent challenges in ensuring universal access to modern contraceptive methods (Statista).
The Government of Nepal has set ambitious targets under Sustainable Development Goal (SDG) 3.7.1 to address family planning needs. By 2022, the goal was for 74% of all women aged 15–49 to have their need for family planning met through modern methods. This target is expected to rise to 80% by 2030 (National Planning Commission, 2020). Achieving these targets is critical for improving maternal and child health outcomes and ensuring gender equality in Nepal.
Despite these efforts, family planning challenges persist in Nepal. According to the Nepal Demographic and Health Survey (NDHS, 2022), 21% of currently married women have an unmet need for family planning services. Furthermore, 57% of currently married women are using some form of contraceptive method, indicating that 78% of currently married women have a demand for family planning services. If all women who expressed a desire to space or limit their children were to adopt family planning methods, the contraceptive prevalence rate would increase from 57% to 78%, highlighting the significant potential to close the gap.
The total demand for family planning that is currently satisfied stands at 73%, with 55% of the total demand being met by modern methods (NDHS, 2022). These statistics reveal a critical need for targeted interventions to enhance access to and utilization of modern contraceptive methods. Efforts to address barriers such as lack of awareness, cultural stigma, and limited healthcare infrastructure are essential to achieving Nepal’s family planning goals and fulfilling the broader commitments of SDG 3.
Reasons for unmet need for Family Planning:
- Limited access to contraceptives: Geographic barriers in rural or remote areas and poor availability of contraceptive supplies and services.
- Limited method choices: Inadequate range of contraceptive options to meet diverse needs.
- Fear or experience of side effects: Concerns about health risks or misconceptions about the safety of contraceptives.
- Cultural or religious opposition: Social norms and religious beliefs discouraging contraceptive use.
- Poor quality of services: Lack of skilled healthcare providers and inadequate counseling and follow-up care.
- Gender-Based barriers: Women lacking autonomy in decision-making and facing partner or family opposition to contraceptive use.
- Provider and user biases: Healthcare providers’ personal biases affecting recommendations and societal stigma around contraceptive use, especially for young or unmarried women.
- Economic constraints: High costs of contraceptive methods or services.
- Youth-specific barriers: Lack of youth-friendly services.
Consequences of unmet need:
- High rates of unintended pregnancies.
- Increased maternal and neonatal mortality.
- Unsafe abortions and related health complications.
- Disruption of educational and economic opportunities, especially for young women.
Emergency Contraception
Emergency Contraception
Emergency contraception refers to methods used to prevent pregnancy after unprotected sex or contraceptive failure, with maximum effectiveness when used as soon as possible after the event. The term “emergency contraception” is preferred over “post-coital contraceptives” as it emphasizes that these methods are not intended for regular use.
In Nepal, two main methods of emergency contraception are available:
- Oral contraceptive pills
- Intrauterine devices (IUDs)
While most contraceptives are designed for use before intercourse, some methods can also be used within a short time after unprotected intercourse, commonly referred to as “morning-after pills.” However, the term “emergency contraceptives” or “secondary contraceptives” is more appropriate.
Mechanism of Action
- Oral contraceptive pills: These work by preventing or delaying ovulation but do not induce an abortion.
- Copper IUD: This device prevents fertilization by causing chemical changes in sperm and eggs before they meet.
Indications for use
Emergency contraception is recommended in the following situations:
- When no contraceptive method has been used.
- In cases of contraceptive accidents or misuse, such as:
- Condom rupture, slippage, or misuse.
- Failed coitus interrupts.
- Miscalculation of the periodic abstinence method.
- IUD expulsion.
- Unprotected sex before the effective time of a vasectomy.
- Failure of a spermicide tablet or film to dissolve.
- When a woman has been a victim of sexual assault.
Method of emergency contraception
| COCs– (Yuzpe method) | Should be taken within 72 hours of unprotected sex and repeated after 12 hours. | COCs low dose (30-33 μg of ethinyl estradiol) Take 4 tablets within 72 hours of unprotected sex (1st dose) Then ↓ Take 4 more tablets after 12 hours (2nd dose) 4+4= Total 8 tablets |
| POPs- (Progestin only pills) | Should be taken within 72 hrs of unprotected sex & repeated after 12 hrs. | POPs (0.75mg Levonorgestrel =1 tablet) e.g. Postinor, e-CON, Contragest, Feminor, Max-72, Pregnon, E-72 Take 1 tab. (0.75 mg) within 72 hrs. of unprotected sex (1st dose) Then ↓ Take 1 more tab. (0.75mg) after 12 hrs. (2nd dose) 1+1=Total 2 tab. (1.5mg) OR ↓ OR POPs (1.5 mg Levonorgestrel=1 tab.) Take 1 tab (1.5mg) of single does within 72 hours of unprotected sex. E.g. i-pill, unwanted -72 OR POPs (0.075 mg Norgestrel=1 tab.) Take 20 tab. within 72 hours (1st dose) Then ↓ Take 20 more tablets after 12 hours (2nd dose) 20+20=40 tablets (3 mg) |
| IUCDs | Should be inserted within 5 days of unprotected intercourse | Counsel client about post insertion bleeding, help her understand how to distinguish this from a menstrual period |
Contraception for special groups
1. Adolescents (10-19 years)
Adolescents experience significant physical, mental, and social changes, which can lead to various sexual and reproductive health challenges, including early marriage, unintended pregnancies, and sexual abuse. Many are sexually active but lack the maturity and knowledge to make informed decisions about contraception, exposing them to risks like STIs, early childbearing, and unsafe abortions.
- Consequences of early and unwanted pregnancy in adolescents:
- Increased maternal and infant mortality rates.
- Higher risk of obstructed labor, preterm birth, low birth weight, and stillbirth.
- Social stigma, limited educational and employment opportunities.
- Unsafe abortions due to lack of access to safe services.
- High vulnerability to STIs, including HIV.
- Family Planning counseling for adolescents:
- Create a safe, confidential, and judgment-free environment.
- Use simple language and provide unbiased, comprehensive information.
- Encourage open discussions and address their reproductive health concerns.
- Contraceptive methods for adolescents:
- Condoms: Most suitable; prevent both pregnancy and STIs.
- COCs: Effective but require proper guidance; do not prevent STIs.
- POPs: Less effective than COCs and do not prevent STIs.
- Injectable (DMPA): Long-term option but may cause side effects like spotting and irregular menstruation.
- IUCDs: Suitable for those without STIs or multiple sexual partners.
- Permanent sterilization: Not suitable for this age group.
2. Women over 35 years
Women over 35 face increased risks associated with pregnancy, including maternal and perinatal mortality, chromosomal abnormalities, and spontaneous abortions. Although fertility declines, contraception is necessary to avoid unintended pregnancies.
- Specific risks in pregnancy over 35:
- Maternal mortality is five times higher than in women in their 20s.
- Perinatal mortality and risks of chromosomal abnormalities (e.g., Down’s syndrome) increase.
- Contraceptive methods for women over 35:
- COCs: Suitable if estrogen levels are low, but not for heavy smokers.
- POPs: Safe for smokers.
- IUCDs: Hormonal and copper devices are effective.
- Condoms: Safe and effective.
- Permanent sterilization: Suitable for those not planning future pregnancies.
3. Post-Abortion contraception
Post-abortion care is critical to prevent repeat unwanted pregnancies and unsafe abortions. Ovulation may resume as early as 11 days after an abortion, necessitating immediate initiation of family planning services.
- Key components of Post-Abortion FP counseling:
- Address reproductive goals and contraceptive needs.
- Provide comprehensive information on methods, effectiveness, and side effects.
- Offer method choice (short-term, long-term, hormonal, or non-hormonal).
- Ensure access to follow-up care and protection against STIs.
- When to start:
- FP services should begin immediately, as ovulation can occur before the next menses.
- Contraceptive methods Post-Abortion:
- COCs/POPs: Safe if no contraindications exist.
- IUCDs: Not suitable if the abortion occurred in the second trimester; delay insertion for four weeks.
- Condoms: Safe and effective.
- Natural methods: Not reliable due to unpredictable ovulation.
- Sterilization: Suitable if no infection; wait until sepsis heals (approximately three months).
By addressing the unique needs of these special groups, effective family planning services can reduce maternal mortality, prevent unsafe abortions, and promote overall reproductive health.
Roles and responsibilities of nurses in the management of Family Planning services
Nurses play a critical role in managing family planning services, contributing to administrative, supervisory, functional, educational, research, and evaluative aspects. Their responsibilities encompass promoting reproductive health, supporting clients, and ensuring effective delivery of family planning programs. Below are the key roles and responsibilities:
1. Administrator
- Nurses in senior positions contribute to organizing family welfare programs at national, provincial, and community levels.
- They assist in developing nursing activities within the framework of family planning programs.
- Responsibilities include managing procedures conducted in family planning services and ensuring the availability of necessary supplies to maintain the continuity of services.
- They collaborate with stakeholders to design and implement effective strategies to meet family planning goals.
2. Supervisor
- Nurses oversee the work of other health workers, new staff, and students, ensuring high-quality service delivery.
- They play a key role in organizing in-service education and training programs for staff to enhance their knowledge and skills in family planning.
- Supervisors monitor staff to identify opportunities for advising mothers or couples on child spacing and family planning methods.
- They encourage adherence to best practices and ethical standards in the delivery of services.
3. Functional Role
- Nurses identify eligible couples and guide them toward adopting appropriate family planning methods.
- Nurses Provide direct health care to clients seeking family planning services.
- Coordinate with team members, clients, and their families to ensure seamless service delivery.
- Act as facilitators, counselors, and advisors, supporting clients in making informed decisions about their reproductive health.
- Offer appropriate suggestions regarding birth control methods tailored to individual needs.
- Maintain client privacy and confidentiality.
- Ensure a welcoming and supportive environment for clients.
- Community Outreach: Nurses coordinate, support, and monitor outreach activities to promote family planning awareness and accessibility in the community.
4. Counselor
- Nurses assist clients in understanding the details of family planning methods, including their benefits, risks, and usage.
- They help clients choose the most suitable contraceptive method and address any concerns or questions.
- Counselors ensure a non-judgmental, client-centered approach and create a supportive environment for decision-making.
- They advocate for informed choices while respecting cultural and personal values.
5. Health Educator
- Nurses play a vital role in educating patients and the community about family planning and reproductive health.
- As a part of counseling in family planning nurses must have sound knowledge of:
- Human biology and reproduction.
- Family life education.
- Concepts and principles of family planning.
- Factors influencing the acceptance of family planning services.
- Available facilities and contraceptive options.
- Nurses effectively deliver education using audiovisual aids and interactive methods in hospitals, health centers, schools, homes, and community settings.
- They promote awareness of fertility, contraception, and the importance of family planning for individual and community health.
6. Researcher
- Nurses are integral members of multidisciplinary research teams and contribute to advancing knowledge and practice in family planning.
- Responsibilities include maintaining accurate records and reports on:
- Methods of contraception used.
- Side effects and contraindications.
- Client compliance and effectiveness of methods.
- These records serve as valuable data for research and evidence-based decision-making.
- Nurses may also participate in studies to evaluate innovative approaches and improve service delivery.
7. Evaluator
- Nurses are actively involved in evaluating the effectiveness of family planning programs and services.
- Evaluation includes:
- Assessing the impact of services on clients and communities.
- Identifying strengths, weaknesses, and gaps in service delivery.
- Analyzing the activities provided by facilitators to ensure alignment with program goals.
- Nurses help establish criteria for measuring achievements and contribute to improving the quality and reach of family planning services.
Responsibilities of a Nurse in Family Planning
- Encouragement and support
- Encourage and support couples who desire a small family.
- Education and counseling
- Educate individuals, couples, and groups on family methods using Information, Education, and Communication tools.
- Counsel clients to address their fears, doubts, and concerns by providing clear information and clarifying misconceptions.
- Help clients choose suitable FP methods based on their needs and preferences by providing accurate information about devices and methods.
- Providing support
- Offer emotional support and guidance to couples to begin and continue the use of FP devices.
- Case finding and follow-up
- Identify couples who need family planning services and conduct follow-ups to ensure their continued use.
- Clinic preparation and maintenance
- Prepare the physical setup for the family planning clinic, including managing clinical areas, arranging examination and waiting rooms, and supervising cleanliness.
- Prepare and sterilize equipment and supplies.
- Infection prevention
- Maintain infection prevention principles during all family planning procedures.
- Staff training and supervision
- Arrange and provide training to staff on new concepts and methods of family planning, including infection prevention.
- Supervise and guide junior staff, students, and subordinates.
- Client preparation and assistance
- Prepare clients for counseling and sterilization procedures.
- Assist surgeons during surgical procedures like laparoscopy, minilap, and vasectomy.
9. Post-operative care
- Provide post-operative care and advise clients on follow-up visits and medication use.
10. Referral services
- Refer clients to appropriate facilities for family planning services if unavailable at the current institute.
- Stay updated on all available services to guide potential clients to suitable facilities.
- Community Involvement
- Organize and participate in mobile camps for family planning.
- Conduct family planning programs and maintain accurate records and reports as per standard protocols.
- Advocacy and awareness
- Raise awareness about family planning services in the community through education, campaigns, and outreach programs.
Sources:
Basavanthappa, B. T. (2008). Community health nursing (2nd ed.). Jaypee Brothers Medical Publishers.
Park, K. (2021). Park’s textbook of preventive and social medicine (26th ed.). Bhanot Publishers.
Retrieved from:
https://my.clevelandclinic.org/health/treatments/4933-tubal-ligation
https://www.who.int/news-room/fact-sheets/detail/family-planning-contraception
https://dhsprogram.com/pubs/pdf/PR142/PR142.pdf
https://censusnepal.cbs.gov.np/results/files/result-folder/National%20Report_English.pdf
https://medicallib.co.za/ml2/fertility-awareness-methods



