
Normal Labour
Introduction
The usual duration of human pregnancy is about 40 weeks, and labor generally takes place between the 37th and 42nd weeks of gestation. Throughout pregnancy, women experience numerous physiological changes that ready them for the experiences of childbirth and motherhood. In the final weeks of pregnancy and at the beginning of labour, intricate physical and emotional changes take place. These changes help ready the woman for the labour and birthing process. As pregnancy reaches its later stages, both the woman’s body and the fetus make preparations for the upcoming labour
The developing fetus has matured to prepare for life outside the womb for extra uterine life. Labour and birth represent the end of pregnancy, the beginning of extra-uterine life for new-born, and a change in the lives of the family. The transition from pregnancy to labour is a sequence of events that begins gradually. Labour is the natural process by which a viable fetus is expelled from the uterus. It varies greatly in duration, severity and risk involved in the mother and fetus.
Labour
Labour is described as the process by which the fetus, placenta and membrane are expelled though the birth canal.
Or
Series of events that take place in the genital organs in an effort to expel the viable products of conception (fetus, placenta and the membranes) out of the womb through the vagina into the outer world is called Labour.
Delivery
Delivery is the expulsion or extraction of a viable fetus out of the womb. It is not synonymous with labour. Delivery can take place without labour as in the elective caesarean section. Delivery may be vaginal, either spontaneous or aided or it may be abdominal.
Expected Date Of Delivery (EDD)
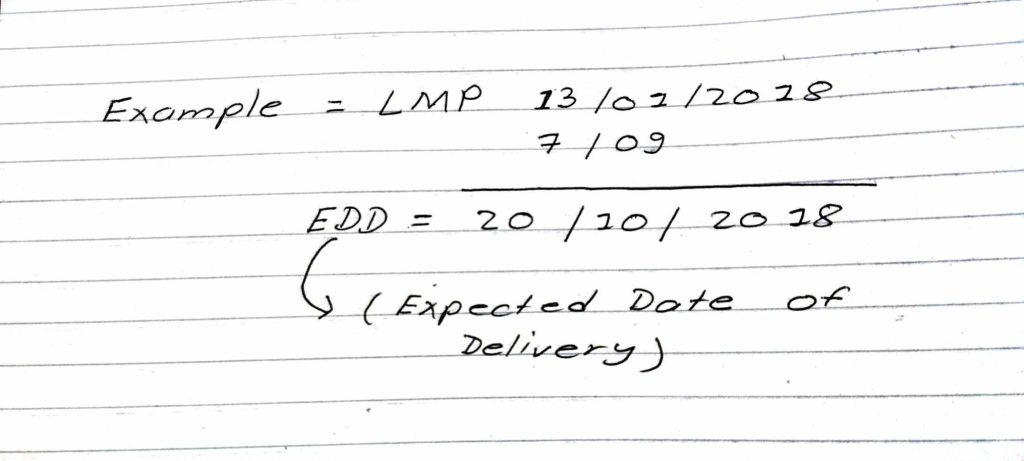
The date of onset of labour cannot be predicted with any accuracy. A calculation based on the date of the last menstruation is the method in common use and is the most accurate method the average duration of pregnancy in woman is 40 weeks or 280 days.
•In practice, the EDD is calculated by adding seven days to the first day of the last menstrual period (LMP) and then counting forward nine calendar months (Negale’s law)
Normal labour
Normal labour is also termed as eutocia. It occurs at term and is spontaneous in onset with the fetus presenting by the vertex. The process is completed with 18 hours and no complications arises.
Normal labour occurs between 37 to 42 weeks’ gestation.
Normal labour is called when it is fulfilling the following criteria;
-Spontaneous in onset and at term
-With vertex presentation
-Without undue prolongation
-Natural termination with minimal aid
-Without having any complications affecting the health of the mother and /or baby.
Abnormal labour (Dystocia)
Any deviation from the definition of normal labour is called abnormal labour. Thus, labour in a case with presentation other than vertex or having some complications even with vertex presentation affecting the course of labour or modifying the nature of termination or adversely affecting the maternal and/or fetal prognosis is called abnormal labour.
False Labour : (false labour, spurious labour)
It is more commonly found in primigravida compared to those of multiparous women. It usually appears prior to the onset of true labour pain by 1 or 2 weeks in primi gravida and by a few days in multipara. These discomforts are likely a result of the cervix and lower uterine segment stretching.
False labour pain is:
- Dull in nature
- Confined to lower abdomen and groin,
- Not associated with hardening of the uterus,
- They have no other features of true labour pain and
- Usually relieved by enema or sedatives
True Labour
True labour is the rhythmic and regular uterine contractions. The interval of contractions is constant and decreases in frequency, the duration and intensity increases over time, and they are unchanged by positional or activity changes.
| True labour | False labour |
| Contraction occur at regular intervals | Contractions occur at irregular interval |
| Intervals between contraction gradually shorten | Interval remain long |
| Intensity gradually increases | Intensity remains unchanged |
| Discomfort is in the back and abdomen | Discomfort is chiefly in the lower abdomen |
| Cervix dilates | Cervical does not dilate |
Physiology of onset of normal labour
During pregnancy, the muscles of the uterus undergo significant growth in size (hypertrophy) and an increase in their number (hyperplasia). This leads to the overall enlargement of the uterus. At full term, which is when the pregnancy is nearing its completion, the length of the uterus measures around 35 cm, including the cervix. The upper part of the uterus, known as the fundus, is wider both from side to side (transversely) and from the front to the back (antero-posteriorly) compared to the lower segment. As a result of these changes, the uterus takes on a shape that resembles either a pear or an egg, known as a pyriform or ovoid shape.
Uterine contraction in labour
Throughout pregnancy there is irregular involuntary spasmodic uterine contractions which are painless (Braxton Hicks), no effect on dilatation of cervix. The character of the contractions changes with the onset of labour. While there are wide variations in frequency, intensity and duration of contractions, remain usually within normal limits in following patterns.
- There is good synchronization of the contraction waves from both halves of the uterus and also between upper and lower uterine segments.
- There is fundal dominance of contractions that diminish gradually in duration through mid-zone down to lower segment.
- The waves of contraction follow a regular pattern.
- The upper segment of the uterus contracts more strongly and for a longer time than the lower part.
- Intra-amniotic pressure rises beyond 20 mm Hg during uterine contraction.
- Good relaxation occurs in between contractions to bring down the intra-amniotic pressure to less than 8 mm Hg.
During contraction, uterus becomes hard and somewhat pushed anteriorly Simultaneously, patient experiences pain which is situated more on the hypogastric region, often radiating to the thighs. Probable causes of pain are:
- Myometrial hypoxia during contractions (as in angina),
- Stretching of the peritoneum over the fundus,
- Stretching of the cervix during dilatation,
- Stretching of the ligaments surrounding the uterus compression of the nerve ganglion.
Tonus: It is intrauterine pressure in between the contractions. During pregnancy as the uterus is relatively inactive the tonus is to 2-3 mmHg. During the first stage of labour it varies from 8-10 mmHg. It is inversely proportional to relaxation. The factors which govern the tonus are;
- contractility of uterine muscles
- intra-abdominal pressure
- over distention of uterus as in twins and polyhydramnios
Intensity: of uterine contraction describes the degree of uterine systole. The intensity gradually increases with advancement of labour until it becomes maximum in 2nd stage during delivery of the baby. Intrauterine pressure is raised to 40–50 mm Hg during 1st stage and about 100–120 mm Hg in 2nd stage of labour during contractions.
In spite of diminished pain in 3rd stage, the intrauterine pressure is probably the same as that in 2nd stage. The diminished pain is due to lack of stretching effect.
Duration: In 1st stage, contractions last for about 30 second. initially but gradually increase in duration with the progress of labour. Thus in 2nd stage, contractions last longer than in 1st stage.
Frequency: In the early stage of labour, contractions come at intervals of 10–15 minutes. The intervals gradually shorten with advancement of labour until in 2nd stage, when it comes every 2–3 minutes.
Retraction of the uterus
In labour where uterine muscle fibers are permanently shortened. Unlike any other muscles of the body, uterine muscles have this property to become shortened.
Contraction is a temporary reduction in length of the fibers, which attain their full length during relaxation. In contrast, retraction results in permanent shortening and the fibers are shortened once and for all.
The net effects of retraction in normal labour are:
- Essential property in the formation of lower uterine segment and dilatation and effacement of the cervix.
- To maintain the descent of the presenting part made by the uterine contractions and to help in ultimate expulsion of the fetus.
- To reduce the surface area of the uterus favouring separation of placenta.
- Effective hemostasis after the separation of the placenta
Stages of labour
Traditionally labour was divided into three stages in which specific development occurs. In recent years a fourth stage has been identified as crucial in the birth process. All stages of labour are carefully observed to assess the progress of normal labour. The average length of first and second stages differ between primigravida and multigravida. However, average length of the third stage and fourth stage are similar of both.
First stage/ dilating stage of labour
It starts from the onset of true labour pain and ends with full dilatation of the cervix. It is, in other words, the “cervical stage” of labour. Its average duration is 12 hours in primi-gravida and 6 hours in multipara.
According to reference manual of SBA (2016), duration in primigravida is 8-10 hours, and in multipara 6-8 hours (DOHS, 2016).
There are three phases in first stage of labour
The latent phase
It is the early, slow part of labour, which begins with the onset of regular contractions and last until cervix is dilated 4 cm. It is prior to active phase of first stage of labour.
It may last 6-8 hours in the first time mother (primigravida), the cervix dilates 0-4 cm and cervical canal shortens from 3 cm long to less than 0.5 cm long.
The uterine contractions occur about every 10-15 minutes and lasts about 15 – 20 seconds. The woman feels that she is able to cope with discomfort. She is often talkative and smiling.
The active phase
The time when the cervix undergoes more rapid dilatation. This begins when the cervix dilates 4 cm and presence of rhythmic uterine contraction. It completes when the cervix is fully dilated (10 cm).
This phase causes the woman different degree of discomfort. The contractions are stronger and last longer, with the result that cervical dilatation progresses. The duration of contraction increases to 30 to 45 seconds and 5 minute apart, and moderate to strong intensity.
During this phase the woman can be assisted in her breathing technique and relaxation. She may continue to ambulate until she is uncomfortable or until membrane rupture. As her contraction increases, her anxiety and discomfort increases.
The transition phase
The last part of the first phase. It is the stage of labour when the cervix is from around 8 to 10 cm dilated.
Cervical dilatation continuous at slower rate but becomes complete. The contractions become more frequent and, longer and stronger.
During this phase, the woman may exhibit decreased ability to cope with her contractions and pain. Often, woman becomes very restless and frequently changing position. It is crucial that nurse should stay with the woman at this time for backup. She may become nauseated and even vomit. She may become irritable and may reject touch during her contractions.
Second stage
It starts from the full dilatation of the cervix (not from the rupture of the membranes) and ends with expulsion of the fetus from the birth canal. Its average duration is 2 hours in primigravida and 30 minute in multigravida.
It has got two phases—
- The propulsive phase—starts from full dilatation up to the descent of the presenting part to the pelvic floor.
- The expulsive phase is distinguished by maternal bearing down efforts and ends with delivery of the baby. Its average duration is 2 hours in primigravida and 30 minutes in multipara.
Third stage
Third stage of labour is referred as placental stage. It begins after birth of the fetus and ends with expulsion of the placenta and membranes (afterbirths). It lasts upto 30 minute with average duration is about 10- 15 minutes in both primigravida and multipara. The duration is reduced to 5 minutes in active management.
Fourth stage
It is the stage of observation for at least 1 hour after expulsion of the afterbirths. During this period, healthcare providers monitor maternal vitals, uterine retraction, and any vaginal bleeding. They also examine the baby. These actions are taken to ensure the well-being of both the mother and the baby.
Normal labour ppt
Download ppt: Click here
For more details: click here
Additional link: click here


You May Also Like
Mechanism of labour
Title: Signs and Symptoms of the Second Stage of Labour
