
Cholecystitis
Cholecystitis is an inflammation of the gallbladder, which is commonly caused by the obstruction of the cystic and common bile ducts by gallstones. This condition leads to the buildup of bile within the gallbladder, causing irritation, swelling, and infection. In some cases, the inflammation may result in complications such as the formation of abscesses, perforation of the gallbladder, or the development of gangrene.
Prevalence
Gallstones, a leading cause of cholecystitis, are present in approximately 10–15% of the general population, with variations across countries. Between 20% and 40% of individuals with gallstones may develop complications such as acute cholecystitis. (WJES, 2020)
Classification
- Acute cholecystitis: Acute cholecystitis is a sudden inflammation of the gallbladder, typically resulting in severe pain in the upper abdomen. It is most commonly caused by gallstones, with at least 95% of cases being associated with the presence of gallstones. The obstruction of the cystic duct by these stones leads to bile buildup, which causes inflammation and infection of the gallbladder.
- Acalculous cholecystitis: Acalculous cholecystitis refers to acute inflammation of the gallbladder that occurs without the presence of gallstones or bile obstruction. This form of cholecystitis is less common but can result from conditions such as sepsis, burns, trauma, or infections that impair blood flow to the gallbladder. It is often more severe and can lead to complications such as gallbladder necrosis or perforation.
- Chronic cholecystitis: Chronic cholecystitis is long-standing inflammation of the gallbladder that typically develops after repeated episodes of acute cholecystitis. Over time, this repeated inflammation leads to the thickening of the gallbladder wall, rigidity, and poor function. The gallbladder may become less efficient at storing and releasing bile, leading to ongoing digestive issues. Chronic cholecystitis is often associated with the presence of gallstones (calculi).
- Calculus cholecystitis: Calculus cholecystitis is inflammation of the gallbladder caused by the obstruction of bile flow due to the presence of gallstones. It is the most common cause of cholecystitis, responsible for more than 90% of cases. The gallstones obstruct the cystic duct, leading to bile retention, inflammation, and infection in the gallbladder.
Causes
- Gallstones (90%) gallstones are the most common cause of cholecystitis, accounting for approximately 90% of cases. When gallstones obstruct the cystic duct or the common bile duct, it leads to the accumulation of bile in the gallbladder, causing inflammation, infection, and sometimes irritation of the gallbladder lining.
- Bile duct blockage of the bile ducts due to gallstones, sludge, or strictures can prevent the normal flow of bile from the gallbladder, leading to inflammation. This condition can increase pressure within the gallbladder, resulting in irritation and infection.
- Tumors or trauma in or around the gallbladder or bile ducts can obstruct bile flow, leading to cholecystitis. Trauma, either from injury or surgery, may also damage the gallbladder or bile ducts, increasing the risk of inflammation and infection.
- Microorganisms (E. coli, bacteroides) infections from microorganisms, such as E. coli or Bacteroides, can contribute to the development of cholecystitis. These bacteria often enter the gallbladder through the bile duct and cause infection, further complicating the condition. Infections are more likely when the bile flow is impaired or when there is a pre-existing obstruction.
Pathophysiology
Chronic cholecystitis typically results from repeated episodes of acute cholecystitis, usually due to the ongoing presence of gallstones. Over time, the gallbladder wall becomes thickened and fibrotic, which reduces its ability to contract and release bile effectively. The repeated cycles of inflammation lead to permanent changes in the gallbladder’s structure and function.
Chronic inflammation triggers mucosal hyperplasia (increased growth of the mucosal lining) and fibrosis (scarring of tissue). These structural changes make the gallbladder less elastic and less efficient at bile storage and secretion. As a result, there may be intermittent symptoms such as dyspepsia (indigestion), nausea, and discomfort, especially after meals.
Although chronic cholecystitis is often asymptomatic, the reduced functionality of the gallbladder can lead to increased risk of further gallstone formation.
Signs and symptoms
- Patients with cholecystitis often experience pain and tenderness in the upper right quadrant of the abdomen, which may radiate to the epigastrium or the right scapula. This pain is typically severe and sharp.
- The pain usually starts suddenly and escalates, reaching its peak intensity within 30 minutes. It may persist or worsen, often causing significant discomfort.
- Nausea and vomiting are common symptoms, occurring in approximately 60-70% of cases. Fever is also frequent, often accompanying the inflammation and infection within the gallbladder.
- Some patients may develop mild jaundice, characterized by yellowing of the skin or eyes, due to bile duct obstruction or liver involvement.
- A positive Murphy’s sign is a key diagnostic feature of cholecystitis. When a healthcare provider palpates the right upper quadrant of the abdomen while the patient takes a deep breath, the patient will often stop breathing due to extreme tenderness and pain. This sudden cessation of breathing indicates acute inflammation in the gallbladder.
Diagnosis
- Liver Function Tests (LFTs): Liver function tests may show increased levels of liver enzymes such as aminotransferases (AST, ALT) and alkaline phosphatase (ALP). Elevated liver enzyme levels suggest liver involvement or bile duct obstruction, which is commonly associated with cholecystitis.
- Blood tests: Blood tests typically show an increase in white blood cell (WBC) counts, which is indicative of an infection or inflammation in the body. The elevation in WBCs is often seen in bacterial infections such as cholecystitis.
- Ultrasonography (USG): Abdominal ultrasonography is one of the most effective imaging techniques to diagnose cholecystitis. It can reveal an enlarged gallbladder, thickening of the gallbladder wall, and the presence of gallstones or bile sludge. Ultrasonography also helps detect any fluid collection or signs of inflammation around the gallbladder.
- Abdominal X-rays: Abdominal X-rays are not always the primary diagnostic tool for cholecystitis but can sometimes show indirect signs, such as an enlarged gallbladder. However, they may not always provide as much detail as an ultrasound.
Prevention
- Maintain a balanced diet by including healthy fats such as those from avocados, fish (salmon, mackerel, and sardines), nuts (almonds and walnuts), seeds (chia seeds and flaxseeds), and olive oil etc.
- Stay hydrated by drinking plenty of water throughout the day to maintain bile consistency and lower the risk of gallstone formation.
- Exercise regularly, as physical activity helps maintain a healthy weight and improves bile circulation.
- Limit alcohol and avoid smoking, as excessive alcohol consumption and smoking can increase the risk of gallbladder disease, including gallstones.
- Include healthy sources of protein, selecting lean proteins like chicken, fish, tofu, and beans instead of high-fat meats, which can raise the risk of gallstones.
- Avoid prolonged hormonal therapy if possible, as long-term use of estrogen-containing medications, such as hormone replacement therapy or certain birth control pills, may increase the risk of gallstones.
- Be aware of family history, and if you have a family history of gallstones, discuss risk factors with a healthcare provider. It may require additional monitoring or preventive measures.
Management
- Hospitalization is often required for patients with cholecystitis, especially those with severe symptoms, dehydration, or complications. Inpatient care allows for close monitoring and immediate treatment.
- Antibiotic therapy is essential if there is an underlying bacterial infection contributing to the cholecystitis. Broad-spectrum antibiotics are typically administered to treat any potential infections and to prevent further complications such as sepsis.
- Analgesics are given to manage pain and discomfort. Common medications include nonsteroidal anti-inflammatory drugs (NSAIDs) or opioids, depending on the severity of pain.
- Antacids may be used if there is gastric irritation or acid reflux related to the illness.
- Comfort measures, including positioning to reduce pain, applying heat to the abdomen, and offering small, frequent meals, can help alleviate symptoms. Bed rest may be recommended for some patients to aid in recovery.
- Patients with cholecystitis, particularly those who are vomiting or have a reduced oral intake, should have their fluid and electrolyte balance monitored carefully. IV fluids may be required to correct dehydration, maintain blood pressure, and support kidney function.
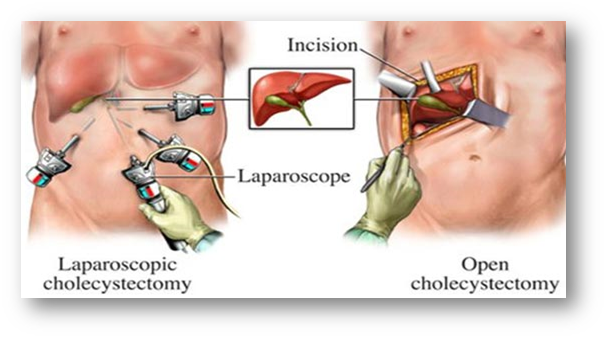
- Surgical intervention – Cholecystectomy
Surgical removal of the gallbladder (cholecystectomy) is the treatment for cholecystitis, particularly in cases where gallstones are the underlying cause. There are two approaches:
- Laparoscopic cholecystectomy: A minimally invasive procedure where small incisions are made, and the gallbladder is removed using a camera and specialized instruments. This method typically results in a shorter recovery time.
- Open cholecystectomy: In some cases, a more traditional surgery may be needed, especially if the condition is complicated or if laparoscopic surgery is not possible.
Nursing Diagnoses
- Acute pain related to (inflammation of the gallbladder/ biliary obstruction/ischemia) as evidenced by patient reports of (pain in the upper right quadrant/tenderness on palpation/guarding, and elevated pain scale).
Goal: The patient will report pain reduction or tolerable pain levels, demonstrating comfort and improved physical activity.
2. Anxiety related to (the uncertainty of diagnosis, pain, and potential complications)
as evidenced by ( restlessness/increased heart rate/verbal expressions of fear/difficulty in making decisions)
Goal: The patient will report decreased anxiety levels and demonstrate effective coping strategies, as evidenced by calm appearance and appropriate responses to stressful situations.
3. Deficient knowledge related to (lack of understanding regarding the disease process/prevention and treatment options) as evidenced by ( questions about the condition/treatment options and lifestyle modifications).
Goal: The patient will demonstrate understanding of the condition, including causes, treatments, and lifestyle changes, as evidenced by verbalization of accurate information.
4. Impaired skin integrity related to: potential gallbladder perforation leading to leakage of bile into the peritoneal cavity, which can cause peritonitis and skin breakdown as evidenced by presence of abdominal distension, signs of infection, and wound site (if surgery is performed).
Goal: The patient will maintain intact skin and tissues, as evidenced by absence of skin breakdown or infection
5. Risk for deficient fluid volume related to (vomiting, fever, decreased oral intake, increased fluid loss (due to diarrhea or sweating) as evidenced by: dehydration signs such as dry mucous membranes, low urine output, and hypotension.
Goal: The patient will maintain adequate fluid balance as evidenced by stable blood pressure, normal skin turgor, and adequate urine output.
6. Risk for imbalanced nutrition: less than body requirements related to: (nausea, vomiting, and discomfort during digestion) as evidenced by: decreased appetite, inadequate caloric intake, and unintentional weight loss.
Goal: The patient will demonstrate adequate nutritional intake and maintain an appropriate body weight, as evidenced by improved appetite and normal weight.
7. Risk for infection related to: presence of gallbladder infection, potential for bacterial growth due to bile stasis, and compromised immune system as evidenced by: fever, elevated white blood cell count, and localized pain.
Goal: The patient will remain free from infection, as evidenced by stable body temperature, normal lab values, and no signs of systemic infection.
8. Risk for electrolyte imbalance related to: vomiting, diarrhea, and inadequate fluid intake as evidenced by: signs of electrolyte disturbances such as muscle cramps, dizziness, and changes in lab results.
Goal: The patient will maintain balanced electrolytes, as evidenced by normal lab values and absence of symptoms like cramping or dizziness.
Complications
- Gallbladder rupture- A severe infection or inflammation can cause the gallbladder wall to weaken and rupture, leading to peritonitis (inflammation of the abdominal cavity).
- Gangrene- Prolonged inflammation may compromise the blood supply to the gallbladder, causing tissue death (gangrene), which increases the risk of rupture.
- Peritonitis- If the gallbladder ruptures, bile and other contents can spill into the abdominal cavity, leading to peritonitis, a life-threatening infection.
- Choledocholithiasis- Gallstones can move into the common bile duct, causing obstruction and leading to cholangitis (bile duct infection) or pancreatitis.
- Biliary fistula- An abnormal connection between the gallbladder and other structures, such as the gastrointestinal tract, may form due to chronic inflammation.
- Chronic cholecystitis- Repeated episodes of acute cholecystitis can lead to chronic inflammation and fibrosis of the gallbladder, impairing its function.
- Gallstone ileus- Large gallstones can erode into the intestine, causing a mechanical bowel obstruction, known as gallstone ileus.
- Mirizzi syndrome- Compression or obstruction of the common bile duct by a gallstone lodged in the cystic duct, leading to jaundice and bile duct inflammation.
- Sepsis Untreated cholecystitis can result in systemic infection (sepsis), which can be life-threatening.
Sources: Waugh, A., & Grant, A. (2012). Ross and Wilson Anatomy and Physiology in Health and Illness (11th ed.). Reed Elsevier India Private Limited.
For additional links:
- https://ajmanavta.com/laparoscopic-surgery/
- https://my.clevelandclinic.org/health/diseases/15265-gallbladder-swelling–inflammation-cholecystitis
- https://www.mayoclinic.org/diseases-conditions/gallstones/symptoms-causes/syc-20354214
- https://wjes.biomedcentral.com/articles/10.1186/s13017-020-00336-x?utm



