Theories and Models in Community Health Nursing
Introduction
Community health nursing plays an important role in promoting health, preventing illness, and improving the well-being of individuals, families, and populations. To guide effective decision-making and service delivery, nurses rely on a variety of theories and models. These frameworks help explain health behaviors, identify health needs, and design appropriate interventions at the community level.
The application of such models not only enhances the planning and evaluation of public health programs but also ensures that care is evidence-based, culturally appropriate, and targeted to specific population needs. Each model or theory offers a unique perspective whether it’s understanding individual motivation for health behavior, the interaction between people and their environment, or the influence of social and policy factors.
These theories and models such as the Health belief model, Epidemiological model, and Leavell and Clark’s levels of prevention serve as foundational tools that guide community health nurses in making informed decisions, delivering care efficiently, and promoting health at multiple levels from individuals to entire populations. They help nurses understand the factors influencing health behaviors, identify health risks, plan appropriate interventions, and measure the effectiveness of community-based programs. By applying these frameworks, nurses are better equipped to address complex health challenges, advocate for policy changes, and empower communities toward better health outcomes.
PRECEDE–PROCEED Model
The PRECEDE–PROCEED model is one of the most widely used frameworks for planning and evaluating public health interventions. Developed by Lawrence W. Green and Marshall W. Kreuter, it guides health professionals to systematically design programs that respond to the real needs of a community.
- PRECEDE stands for Predisposing, Reinforcing, and Enabling Constructs in Educational Diagnosis and Evaluation. This part is focused on assessment and diagnosis. It begins with identifying social problems affecting the community’s quality of life (social diagnosis). Then, epidemiological data is used to identify the health problems contributing to these social issues (epidemiological diagnosis). After that, behavioral and environmental factors causing the health problems are analyzed. Following this, predisposing factors (knowledge, attitudes), enabling factors (resources, skills), and reinforcing factors (feedback, rewards) that affect behaviors are identified. Finally, administrative and policy issues are considered to understand the practical aspects of program implementation.
- PROCEED stands for Policy, Regulatory, and Organizational Constructs in Educational and Environmental Development. This part covers the actual implementation of the intervention and its evaluation. It includes the implementation of the planned intervention, process evaluation (assessing if the program is delivered as intended), impact evaluation (assessing the immediate effects), and outcome evaluation (assessing long-term health outcomes).
This model ensures interventions are tailored to the specific needs of a community by emphasizing thorough assessment before planning. For example, a nurse aiming to reduce childhood obesity would first gather data about the social factors (like family income or cultural habits), prevalence of obesity, and behavioral factors (e.g. physical inactivity or unhealthy diet). After identifying these, the nurse designs an education program focused on promoting physical activity and healthy eating while addressing environmental barriers like lack of playgrounds or availability of junk food. The nurse also plans to evaluate the effectiveness by tracking changes in BMI and physical activity levels over time.
The PRECEDE–PROCEED model’s strength lies in its comprehensive and systematic approach, incorporating multi-level factors and ongoing evaluation, which helps in developing sustainable and evidence-based public health programs.
Health Belief Model (HBM)
The Health Belief Model (HBM), developed in the 1950s by social psychologists Hochbaum, Rosenstock, and Kegels, focuses on the individual’s perceptions and attitudes as determinants of health behavior. It is one of the earliest models developed to explain why people fail to adopt disease prevention strategies or screening tests.
Key components:
- Perceived susceptibility: The individual’s belief about the risk of acquiring a disease or health condition.
- Perceived severity: How serious the individual believes the consequences of the condition are.
- Perceived benefits: The individual’s belief in the effectiveness of the advised action to reduce risk or severity.
- Perceived barriers: The perceived obstacles that prevent the individual from taking action.
- Cues to action: External or internal triggers that prompt the individual to act, such as health campaigns, advice from others, or symptoms.
- Self-efficacy: Confidence in one’s ability to successfully perform the behavior.
Nurses use HBM to design health education and counseling that address specific beliefs influencing health behaviors. For example, in a tuberculosis (TB) prevention program, a nurse may assess whether community members believe they are at risk for TB (susceptibility), understand how serious untreated TB can be (severity), recognize that getting tested and treated can cure the disease (benefits), and identify barriers such as fear of stigma or cost of treatment. The nurse would then provide information to address misconceptions, reduce barriers (such as linking to free testing services), and offer reminders (cues to action) to increase screening and treatment compliance. Enhancing self-efficacy might involve teaching patients how to take medications properly or manage side effects. This model is particularly useful in individualized counseling, vaccination campaigns, and encouraging participation in preventive health services.
Epidemiological Model
The Epidemiological model, often represented as the epidemiologic triad, is fundamental in understanding the causes, transmission, and control of diseases. It focuses on the interaction between three key components:
- Agent: The biological, chemical, or physical factor that causes disease (e.g., bacteria, viruses, toxins).
- Host: The living organism, usually a human, that can be infected or affected by the agent.
- Environment: The external factors that affect the agent and the opportunity for exposure or transmission (e.g., climate, sanitation, population density).
Disease occurs when there is a susceptible host, a pathogenic agent, and a conducive environment.
This model guides nurses in outbreak investigation, surveillance, and designing control measures. For instance, during a dengue fever outbreak, the nurse identifies the Aedes mosquito as the agent, the human as the host, and the environment as areas with stagnant water that provide mosquito breeding grounds. The nurse educates the community on eliminating standing water, uses insecticide spraying, and collaborates with local health authorities. This comprehensive approach helps interrupt the disease transmission cycle.
Beyond communicable diseases, the model can also be applied to chronic diseases by identifying risk factors (agents) and modifying the environment or behaviors of the host.
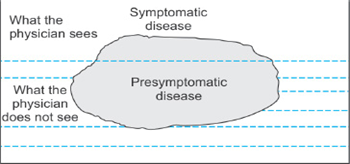
Iceberg Theory of Disease
The Iceberg Theory in public health illustrates that the visible cases of a disease (those diagnosed and symptomatic) are only a small fraction of the total number of cases in the community. The larger, hidden part of the iceberg consists of subclinical or asymptomatic cases, undiagnosed individuals, and those at risk but not yet affected.
This concept emphasizes the importance of active case finding and screening programs. For example, many individuals with hypertension feel well and remain undiagnosed until complications develop. By conducting blood pressure screenings in the community, nurses uncover “hidden” cases early, allowing timely interventions to prevent stroke or heart disease. Similarly, screenings for diabetes, anemia, and malnutrition reveal a large pool of individuals who require preventive or curative care but are unaware of their condition. The Iceberg Theory encourages nurses to move beyond waiting for patients to seek care and proactively identify health problems in the community.
Leavell and Clark’s Levels of Prevention
This classic model divides disease prevention into three levels, each targeting a different stage in the natural history of disease:
- Primary prevention: Actions to prevent the initial occurrence of disease by reducing risk factors or increasing resistance (e.g., immunizations, health education, sanitation).
- Secondary prevention: Early detection and treatment to halt or slow disease progression (e.g., screenings for cancer, hypertension, tuberculosis).
- Tertiary prevention: Measures aimed at reducing disability, restoring function, and preventing complications in individuals with established disease (e.g., rehabilitation, chronic disease management).
Community health nurses utilize all three levels in their practice. For example, primary prevention activities include teaching handwashing and conducting immunization drives. Secondary prevention involves organizing regular health camps for early detection of diabetes or hypertension. Tertiary prevention includes home visits to support stroke survivors, teaching families about medication adherence, and physical therapy exercises.
This model provides a clear framework to deliver comprehensive care that spans from health promotion to chronic disease management.
Milio’s Framework for Prevention
Nancy Milio’s Framework challenges the notion that individual health behaviors are solely a matter of personal choice. She argued that social, economic, and policy environments play a powerful role in shaping people’s health behaviors by creating opportunities and barriers.
Key Points:
- People’s health choices depend on the options available in their environment.
- Effective prevention must address social determinants such as poverty, education, and access to healthy foods.
- Policy changes and environmental improvements are crucial for long-lasting health promotion.
For example, instead of only advising individuals to eat healthy, a nurse may work with schools to implement policies that provide nutritious meals and collaborate with local governments to improve food accessibility in low-income neighborhoods. The nurse might also advocate for policies that promote physical activity, such as safe parks and pedestrian-friendly streets.
Milio’s framework encourages nurses to engage in community organizing, policy advocacy, and creating supportive environments that enable healthy behaviors on a population level.
Salmon White’s Construct for Public Health Nursing
Salmon White’s Construct outlines the essential roles of public health nursing, emphasizing a holistic and collaborative approach:
- Prevention: Actions to avoid disease and injury through education, immunization, and risk reduction.
- Protection: Safeguarding individuals and communities from health hazards, including environmental threats and infectious diseases.
- Promotion: Enhancing overall well-being through health education, lifestyle support, and empowerment.
Nurses operating within this framework provide immunizations, conduct hygiene and sanitation campaigns, report and manage communicable disease outbreaks, and support vulnerable groups such as the elderly, disabled, and low-income families. The approach encourages nurses to build partnerships with individuals, families, and community organizations to address health comprehensively.
Theory of Reasoned Action
Developed by Martin Fishbein and Icek Ajzen, the Theory of Reasoned Action explains that an individual’s behavior is directly influenced by their intention to perform that behavior. This intention is shaped by:
- Attitude: The person’s positive or negative evaluation of the behavior.
- Subjective norms: The perceived social pressure from important people (family, friends, community) to perform or not perform the behavior.
When designing health promotion interventions, nurses can influence both the attitudes and subjective norms. For example, in family planning education, the nurse may not only counsel the woman but also involve her spouse and family members to create a supportive environment. Changing social norms and beliefs about contraceptive use can increase acceptance and practice.
Sources
Park, K. (2021). Park’s textbook of preventive and social medicine (26th ed.). Bhanot Publishers.
https://currentnursing.com/nursing_theory/psychosocial_models_nursing_hbm.html
https://currentnursing.com/nursing_theory/theories_community_health_nursing.html